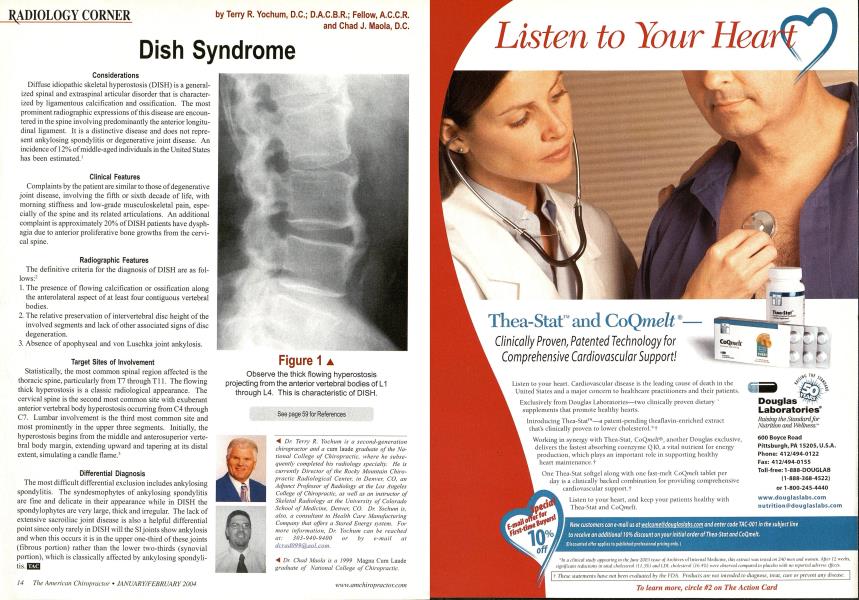
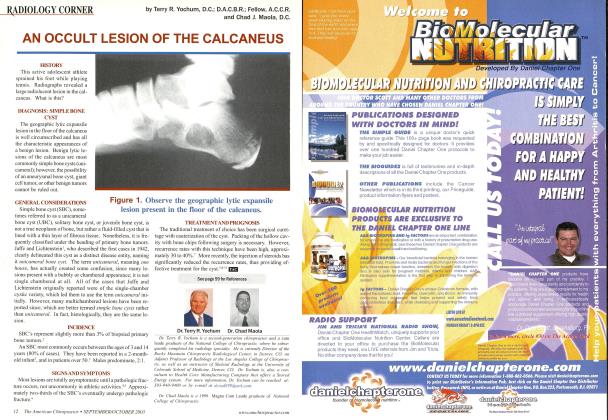
Considerations Diffuse idiopathic skeletal hyperostosis (DISH) is a generalized spinal and extraspinal articular disorder that is characterized by ligamentous calcification and ossification. The most prominent radiographic expressions of this disease are encountered in the spine involving predominantly the anterior longitudinal ligament. It is a distinctive disease and does not represent ankylosing spondylitis or degenerative joint disease. An incidence of 12% of middle-aged individuals in the United States has been estimated.1 Clinical Features Complaints by the patient are similar to those of degenerative joint disease, involving the fifth or sixth decade of life, with morning stiffness and low-grade musculoskeletal pain, especially of the spine and its related articulations. An additional complaint is approximately 20% of DISH patients have dysph-agia due to anterior proliferative bone growths from the cervical spine. Radiographic Features The definitive criteria for the diagnosis of DISH are as follows:2 The presence of flowing calcification or ossification along the anterolateral aspect of at least four contiguous vertebral bodies. The relative preservation of intervertebral disc height of the involved segments and lack of other associated signs of disc degeneration. Absence of apophyseal and von Luschka joint ankylosis. Target Sites of Involvement Statistically, the most common spinal region affected is the thoracic spine, particularly from T7 through Tl 1. The flowing thick hyperostosis is a classic radiological appearance. The cervical spine is the second most common site with exuberant anterior vertebral body hyperostosis occurring from C4 through C7. Lumbar involvement is the third most common site and most prominently in the upper three segments. Initially, the hyperostosis begins from the middle and anterosuperior vertebral body margin, extending upward and tapering at its distal extent, simulating a candle flame.3 Differential Diagnosis The most difficult differential exclusion includes ankylosing spondylitis. The syndesmophytes of ankylosing spondylitis are fine and delicate in their appearance while in DISH the spondylophytes are very large, thick and irregular. The lack of extensive sacroiliac joint disease is also a helpful differential point since only rarely in DISH will the SI joints show ankylosis and when this occurs it is in the upper one-third of these joints (fibrous portion) rather than the lower two-thirds (synovial portion), which is classically affected by ankylosing spondylitis.I See page 59 for References A Dr. Terry R. Yochum is a second-generation chiropractor and a cum laude graduate of the National College of Chiropractic, where he subsequently completed his radiology specialty. He is currently Director of the Rock}- Mountain Chiropractic Radiological Center, in Denver, CO, an Adjunct Professor of Radiology at the Los Angeles College of Chiropractic, as well as an instructor of Skeletal Radiology at the University of Colorado School of Medicine, Denver, CO. Dr. Yochum is, also, a consultant to Health Care Manufacturing Company that offers a Stored Energy system. For more information. Dr. Yochum can be reached at: 303-940-9400 or by e-mail at da:adiiSSI^aa Leo m. •^ Dr. Chad Maola is a 1999 Magna Cum Laude graduate of National College of Chiropractic. Figure 1 Observe the thick flowing hyperostosis projecting from the anterior vertebral bodies of L1 through L4. This is characteristic of DISH.