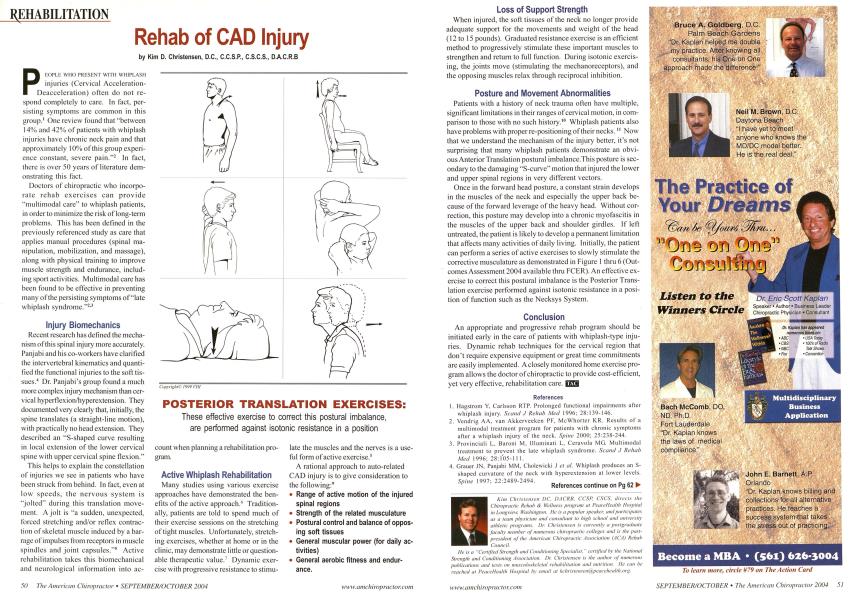
P i i:opli; who pri;sf.nt with whiplash injuries (Cervical Acceleration-Deacceleration) often do not respond completely to care. In fact, persisting symptoms are common in this group.1 One review found that "between 14% and 42% of patients with whiplash injuries have chronic neck pain and that approximately 10% of this group experience constant, severe pain."2 In fact, there is over 50 years of literature demonstrating this fact. Doctors of chiropractic who incorporate rehab exercises can provide "multimodal care" to whiplash patients, in order to minimize the risk of long-term problems. This has been defined in the previously referenced study as care that applies manual procedures (spinal manipulation, mobilization, and massage), along with physical training to improve muscle strength and endurance, including sport activities. Multimodal care has been found to be effective in preventing many of the persisting symptoms of "late whiplash syndrome."2-' Injury Biomechanics Recent research has defined the mechanism of this spinal injury more accurately. Panjabi and his co-workers have clarified the intervertebral kinematics and quantified the functional injuries to the soft tissues.4 Dr. Panjabi's group found a much more complex injury mechanism than cervical hyperflexion/hyperextension. They documented very clearly that, initially, the spine translates (a straight-line motion), with practically no head extension. They described an "S-shaped curve resulting in local extension of the lower cervical spine with upper cervical spine flexion." This helps to explain the constellation of injuries we see in patients who have been struck from behind. In fact, even at low speeds, the nervous system is "jolted" during this translation movement. A jolt is "a sudden, unexpected, forced stretching and/or reflex contraction of skeletal muscle induced by a barrage of impulses from receptors in muscle spindles and joint capsules."5 Active rehabilitation takes this biomechanical and neurological information into ac- count when planning a rehabilitation program. Active Whiplash Rehabilitation Many studies using various exercise approaches have demonstrated the benefits of the active approach.'1 Traditionally, patients are told to spend much of their exercise sessions on the stretching of tight muscles. Unfortunately, stretching exercises, whether at home or in the clinic, may demonstrate little or questionable therapeutic value.7 Dynamic exercise with progressive resistance to stimu- late the muscles and the nerves is a useful form of active exercise.8 A rational approach to auto-related CAD injury is to give consideration to the following:' Range of active motion of the injured spinal regions Strength of the related musculature Postural control and balance of oppos ing soft tissues General muscular power (for daily ac tivities) General aerobic fitness and endur ance. Loss of Support Strength When injured, the soft tissues of the neck no longer provide adequate support for the movements and weight of the head (12 to 15 pounds). Graduated resistance exercise is an efficient method to progressively stimulate these important muscles to strengthen and return to full function. During isotonic exercising, the joints move (stimulating the mechanoreceptors), and the opposing muscles relax through reciprocal inhibition. Posture and Movement Abnormalities Patients with a history of neck trauma often have multiple, significant limitations in their ranges of cervical motion, in comparison to those with no such history.1" Whiplash patients also have problems with proper re-positioning of their necks. " Now that we understand the mechanism of the injury better, it's not surprising that many whiplash patients demonstrate an obvious Anterior Translation postural imbalance.This posture is secondary to the damaging "S-curve" motion that injured the lower and upper spinal regions in very different vectors. Once in the forward head posture, a constant strain develops in the muscles of the neck and especially the upper back because of the forward leverage of the heavy head. Without correction, this posture may develop into a chronic myofascitis in the muscles of the upper back and shoulder girdles. If left untreated, the patient is likely to develop a permanent limitation that affects many activities of daily living. Initially, the patient can perform a series of active exercises to slowly stimulate the corrective musculature as demonstrated in Figure 1 thru 6 (Outcomes Assessment 2004 available thru FCER). An effective exercise to correct this postural imbalance is the Posterior Translation exercise performed against isotonic resistance in a position of function such as the Necksys System. Conclusion An appropriate and progressive rehab program should be initiated early in the care of patients with whiplash-type injuries. Dynamic rehab techniques for the cervical region that don't require expensive equipment or great time commitments are easily implemented. A closely monitored home exercise program allows the doctor of chiropractic to provide cost-efficient, yet very effective, rehabilitation care. E3 References Hagstrom Y. Carlsson RTP. Prolonged functional impairments after whiplash injury. ScamlJ Rehab Meet 1996: 28:139-146. Vcndrig AA. van Akkerveeken PF. McWhorter KR. Results of a multimodal treatment program for patients with chronic symptoms after a whiplash injury of the neck. Spine 2000: 25:238-244. Provinciali L. Baruni M. Illuminati L. Ceravola MG. Multimodal treatment to prevent the late whiplash syndrome. Scaml .1 Rehab Mecl 1996: 28:105-1 1 I. Grauer JN. Panjabi MM. C'holewicki J el cil. Whiplash produces an S- shaped curvature of the neck with hyperextension at lower levels. Spine 1997; 22:2489-2494. ' . References continue on Pg 62 ► Kim Chris tenscn DC. OACRB. CCSP, CSCS. directs the Chiropractic Rehab & It'ellness program at Peace/lealth Hospital in Longview. Washington, He is a popular speaker, and participates as a team physician and consultant to high school and university athletic programs. Dr. Christensen is currently a postgraduate faculty member of numerous chiropractic colleges and i.\ the past-president of the American Chiropractic Association (ACA) Rehab Council. He is a "Certified Strength and C 'auditioning Specialist, " certified by the National Strength and Conditioning Association. Dr. Cltri.stensen is the author of numerous publications and texts on musculoskeletal rehabilitation and nutrition. He can be reached at I'eaceHealth Hospital by email at kchristensenla peacehealth.org.