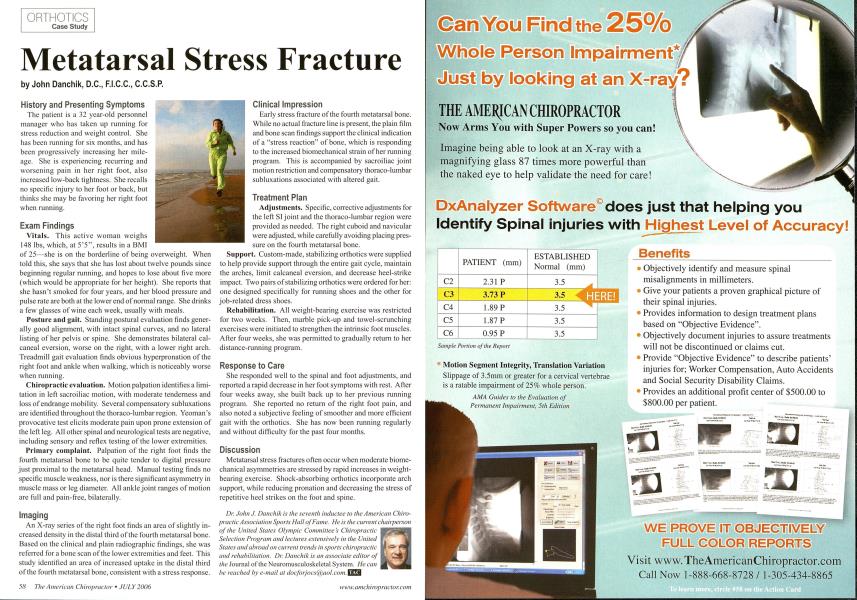
History and Presenting Symptoms The patient is a 32 year-old personnel manager who has taken up running for stress reduction and weight control. She lias been running for six months, and has been progressively increasing her mileage. She is experiencing recurring and worsening pain in her right foot, also increased low-back tightness. She recalls no specific injury to her foot or back, but thinks she may be favoring her right foot when running. Exam Findings Vitals. This active woman weighs 148 lbs, which, at 5'5", results in a BMI of 25—she is on the borderline of being overweight. When told this, she says that she has lost about twelve pounds since beginning regular running, and hopes to lose about five more (which would be appropriate for her height). She reports that she hasn't smoked for four years, and her blood pressure and pulse rate are both at the lower end of normal range. She drinks a few glasses of wine each week, usually with meals. Posture and gait. Standing postural evaluation finds generally good alignment, with intact spinal curves, and no lateral listing of her pelvis or spine. She demonstrates bilateral cal-cancal eversion, worse on the right, with a lower right arch. Treadmill gait evaluation finds obvious hyperpronation of the right foot and ankle when walking, which is noticeably worse when running. Chiropractic evaluation. Motion palpation identifies a limitation in left sacroiliac motion, with moderate tenderness and loss of endrange mobility. Several compensatory subluxations are identified throughout the thoraco-lumbar region. Yeoman's provocative test elicits moderate pain upon prone extension of the left leg. All other spinal and neurological tests are negative, including sensory and reflex testing of the lower extremities. Primary complaint. Palpation of the right foot finds the fourth metatarsal bone to be quite tender to digital pressure just proximal to the metatarsal head. Manual testing finds no specific muscle weakness, nor is there significant asymmetry in muscle mass or leg diameter. All ankle joint ranges of motion are full and pain-free, bilaterally. Imaging An X-ray series of the right foot finds an area of slightly increased density in the distal third of the fourth metatarsal bone. Based on the clinical and plain radiographic findings, she was referred for a bone scan of the lower extremities and feet. This study identified an area of increased uptake in the distal third of the fourth metatarsal bone, consistent with a stress response. Clinical Impression Early stress fracture of the fourth mctatarsal bone. While no actual fracture line is present, the plain film and bone scan findings support the clinical indication of a "stress reaction" of bone, which is responding to the increased biomechanical strain of her running program. This is accompanied by sacroiliac joint motion restriction and compensatory thoraeo-lumbar subluxations associated with altered gait. Treatment Plan Adjustments. Specific, corrective adjustments for the left SI joint and the thoraeo-lumbar region were provided as needed. The right cuboid and navicular were adjusted, while carefully avoiding placing pressure on the fourth metatarsal bone. Support. Custom-made, stabilizing orthotics were supplied to help provide support through the entire gait cycle, maintain the arches, limit calcaneal eversion, and decrease heel-strike impact. Two pairs of stabilizing orthotics were ordered for her: one designed specifically for running shoes and the other for job-related dress shoes. Rehabilitation. All weight-bearing exercise was restricted for two weeks. Then, marble pick-up and towel-scrunching exercises were initiated to strengthen the intrinsic foot muscles. After four weeks, she was permitted to gradually return to her distance-running program. Response to Care She responded well to the spinal and foot adjustments, and reported a rapid decrease in her foot symptoms with rest. After four weeks away, she built back up to her previous running program. She reported no return of the right foot pain, and also noted a subjective feeling of smoother and more efficient gait with the orthotics. She has now been running regularly and without difficulty for the past four months. Discussion Metatarsal stress fractures often occur when moderate biome-chanical asymmetries are stressed by rapid increases in weight-bearing exercise. Shock-absorbing orthotics incorporate arch support, while reducing pronation and decreasing the stress of repetitive heel strikes on the foot and spine. Dr. JohnJ. Danchik is the seventh inductee to the American Chiropractic Association Sports Hall of Fume. He is the current chairperson oj the United Stales Olympic Committee's Chiropractic Selection Program and lectures extensively in the United States and abroad on current trends in sports chiropractic and rehabilitation. Dr. Danchik is an associate editor of the Journal of the Ncuromusculoskelctal System. He can be reached by e-mail at [email protected]. \