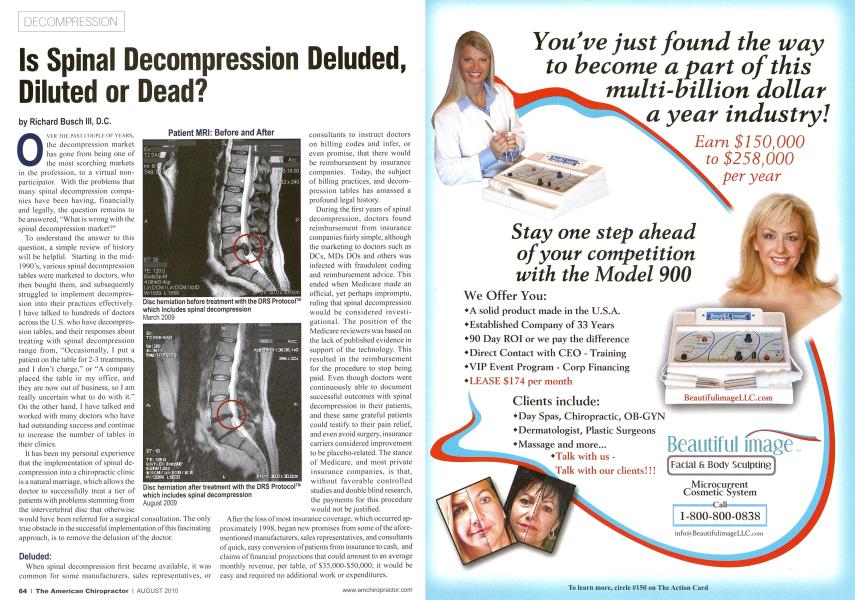
O\t:k tiii: pasi coupu: or yi-:ars, the decompression market has gone from being one of the most scorching markets in the profession, to a virtual non-participalor. With the problems that many spinal decompression companies have been having, financially and legally, the question remains to be answered, "What is wrong with the spinal decompression market?" To understand the answer to this question, a simple review of history will be helpful. Starting in the mid-1990's, various spinal decompression tables were marketed to doctors, who then bought them, and subsequently struggled to implement decompression into their practices effectively. I have talked to hundreds of doctors across the U.S. who have decompression tables, and their responses about treating with spinal decompression range from, "Occasionally, I put a patient on the table for 2-3 treatments, and I don't charge," or "A company placed the table in my office, and they are now out of business, so I am really uncertain what to do with it." On the other hand. 1 have talked and worked with many doctors who have had outstanding success and continue to increase the number of tables in their clinics. It has been my personal experience that the implementation of spinal decompression into a chiropractic clinic is a natural marriage, which allows the doctor to successfully treat a tier of patients with problems stemming from the intervertebral disc that otherwise would have been referred for a surgical consultation. The only true obstacle in the successful implementation of this fascinating approach, is to remove the delusion of the doctor. Deluded: When spinal decompression first became available, it was common for some manufacturers, sales representatives, or consultants to instruct doctors on billing codes and inter, or even promise, that there would be reimbursement by insurance companies. Today, the subject of billing practices, and decompression tables has amassed a profound legal history. During the first years of spinal decompression, doctors found reimbursement from insurance companies fairly simple, although the marketing to doctors such as DCs, MDs DOs and others was infected with fraudulent coding and reimbursement advice. This ended when Medicare made an official, yet perhaps impromptu, ruling that spinal decompression would be considered investi-gational. The position of the Medicare reviewers was based on the lack of published evidence in support of the technology. This resulted in the reimbursement for the procedure to stop being paid. Even though doctors were continuously able to document successful outcomes with spinal decompression in their patients, and these same grateful patients could testify to their pain relief, and even avoid surgery, insurance carriers considered improvement to be placebo-related. The stance of Medicare, and most private insurance companies, is that, without favorable controlled studies and double blind research, the payments for this procedure would not be justified. After the loss ofmost insurance coverage, which occurred approximately 1998. began new promises from some of the aforementioned manufacturers, sales representatives, and consultants of quick, easy conversion of patients from insurance to cash, and claims of financial projections that could amount to an average monthly revenue, per table, of S35.OOO-S5O.OOO; it would be easy and required no additional work or expenditures. The evolution of broken promises in decompression went from easy insurance reimbursement to outrageous profits for little work. Some promises included companies placing tables within a practice for a percentage of fees collected by the doctor for the use of the table. However their agreements were worded, this appears to be fee-splitting which, of course, is illegal. And other promises were made by some companies and/or their representatives who promoted the use of multiple physical therapy codes and even surgical codes which proved to be false. Fraudulent coding resulted in very large fines to good, yet deluded, doctors who believed the advice, both verbal and written, of those who just wanted to sell a spinal decompression table. According to the Anesthesia and Pain Coders Pink Sheet, the general industry reply was summed up by one billing consultant. "Recommending codes is a common practice in the industry... It's up to the physician or coder to decide what is actually best." Several doctors were convicted, and many doctors had to pay major tines. Through all of this delusion, there are doctors who have successfully implemented spinal decompression into their offices - without insurance reimbursement, and thousands of patients with serious disc conditions who have been helped dramatically with their pain - without surgery. Dilution Now, after the delusion, it is unfortunate that there has been a dramatic shift in the mindset of some doctors and some manufacturers about the treatment category of spinal decompression. Even the marketing pendulum seems to swing toward the dilution and diminishment of the value of decompression. There are consultants and companies advocating that decreasing the number of treatments and cutting back the treatment time per session is the way to go. And some are recommending trial-treatments offered for free. There is also the recommendation, which many are taking, "Let us all just categorize spinal decompression as 'traction'; then we all can achieve reimbursement of an average of SI 4.00 per treatment." The perceived value of spinal decompression will become diluted ifthe classification and the difference between the two categories of tables are not allowed to exist, or the line is so blurred that it allows the insurance companies to paint with such a broad brush that it forces the true decompression tables into the same classification as the traction tables. There are significant differences between spinal decompression and traction, just as there are significant difterences between chiropractic and massage therapy or an X-ray and a CT scan, even though there are some similarities. The primary difference between spinal decompression and traction is the ability of spinal decompression to overcome the body's defensive mechanism of muscle guarding, or muscle spasms, by the ramping of the force, or the introduction of a computerized distinctive, specific force over a logarithmic wave. This force can create a negative intradiscal pressure, and this negative in-tradiscal pressure allows the introduction of water, oxygen and nutrients into the disc, allowing it to heal from the inside out. There have been studies that discount the efficacy of traditional traction for the treatment of herniated and degenerative discs1', and there have been studies performed demonstrat- ing the success of spinal decompression for the same type of conditions.2A Unfortunately, many of the decompression studies (with the exception of a study by Vax-D) have not been performed as double blind studies. Additionally, there are not an adequate number of studies performed with other tables that could be regarded as decompression specific, to influence insurance companies to reconsider their ruling. Fortunately this dilution does not have to make decompression therapy a moot point. A doctor in a cash practice, one that is able to exercise best healthcare practices rather than best insurance practices, is able to offer spinal decompression as a viable alternative to sending a patient out for surgery or other invasive tests and procedures. Dead A final question - is spinal decompression dead? 1 only raise this topic since I talk with hundreds of doctors across the country each year about how to implement a cash practice and spinal decompression, and some are very disillusioned doctors who believe decompression is dead. They don't believe there is a future for spinal decompression because of factors covered in this article. Many have just never learned how to do cash, or they don't believe their services are worth the fees they charge, or they are fearful to ask their patients, those who have been used to paying little and the doctor accepting their insurance, to pay for their care; along with that problem some doctors just don't know how to effectively treat with spinal decompression. The effectiveness of decompression is unre-proachable. in my fourteen years of experience. The experience of others who have learned to implement it properly, and decompression's marriage with chiropractic will certainly be a long and lasting union. For the sake of discussion, we know people still have herni-ated and degenerative disc conditions, and up to the writing of this article, there is not a cure, or a way to completely eradicate disc-related conditions. These patients are going somewhere for help, and most would rather choose a non-invasive, pain-free successful treatment. A treatment that can keep a patient working and one that has no potential negative side-effects. They will be seeking spinal decompression. Spinal decompression is not dead; in fact, 1 know that bigger times are yet to come. Dr. Richard E. Busch III is a nationally recognized Doctor of Chiropractic, author, and speaker. He has successfully treated thousands of patients for chronic and severe disc conditions that traditionally would haw required surgery. Dr. Busch developed the DRS Protocol'", utilizing spinal decompression technology. He has served as a national consultant for the continuing development of this technology andthe DRS Protocol™. Dr. Busch has published a recent eye-opening hook *Surgcry not Included: Freedom from Chronic Neck and Back Pain. You can visit his website at www.allcashacademv.com or www.huschchiropractic.coni or call I-H66-662-2225. References: 1. Anderson.H. J. (iunnar, Shull/, A.B. I9NX Intervertebral Disc Pressure During Traction Scandinavian Journal o)'Rehabilitation McJicinc SnpplenwniM-.M-V I. 2. Beattie, P.l:.. Nelson R.M.. Michener 1..A.. Camarrata. J.. Donley, .U200K). Protocols after a prone lumbar traction protocol.....trehives of Physical Mcilicinc ami Rehabilitation. X1), 269-274. 3. Pellechia. Cieralidine. {I t>t)4). Lumbar traction: a review of the literature. Journal of Orrho-pacdic ami Spoils I'/nwical Therapy. Vol.20 (51 262-267. 4. Ramos Ci, Martin W I9l>4. LilVeetsorVericbral Axial Decompression on Intradiscal Pressure. n!f8 Disc herniation before treatment with the DRS Protocol which includes spinal decompression March 2009 Disc herniation after treatment with the DRS Protocol which includes spinal decompression August 2009