Pes Anserine Bursitis
ORTHOTICS
Mark Charrette
Pes anserine bursitis is the result of inflammation of a bursal sac at the medial aspect of the knee. The pes anserinus is the anatomic term used to identify the insertion of the conjoined tendons sartorius, gracilis, and semitendinosus into the anteromedial proximal tibia.
This type of bursitis is a fairly common finding, but it is often overlooked and not very prevalent in literature. There aie many causes of this type of bursitis, but pronation of the feet should be suspected and evaluated.
The patient may volunteer information in the history, such as that he or she has been experiencing medial knee pain after taking a long walk or hike. Doctors of chiropractic must be aware of the possibility of patients presenting to them with knee pain, and they must be able to differentiate and address the problem. This problem may be confused with other knee conditions.
Custom-made, flexible functional orthotics can reduce the effects of medial knee pain, specifically over the pes anserine bursa, and should be used specifically to care for this malady.
Anatomical Considerations
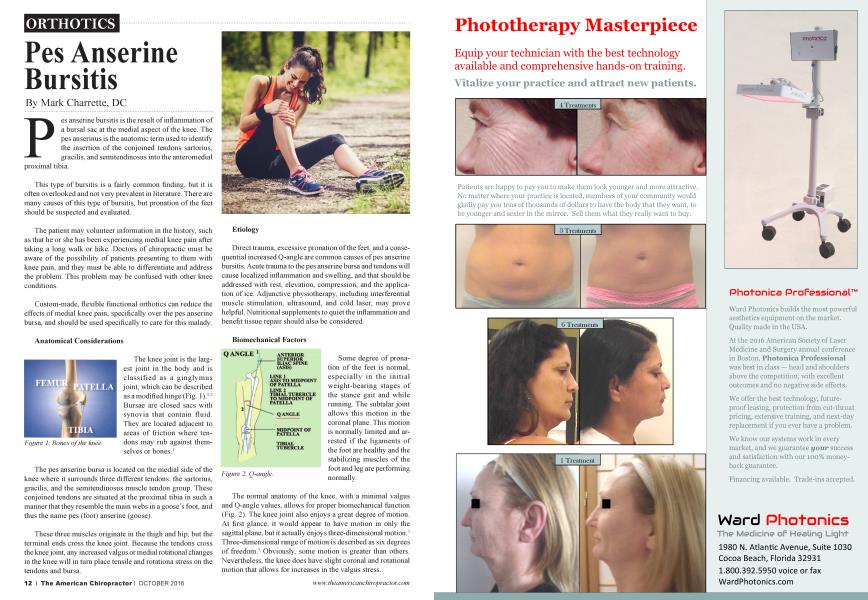
The knee joint is the largest joint in the body and is classified as a ginglymus joint, which can be described as a modified hinge (Fig. I).1-2 Bursae aie closed sacs with synovia that contain fluid. They are located adjacent to areas of friction where tendons may rub against themselves or bones.1
The pes anserine bursa is located on the medial side of the knee where it surrounds three different tendons: the sartorius, gracilis, and the semitendinosus muscle tendon group. These conjoined tendons are situated at the proximal tibia in such a manner that they resemble the main webs in a goose’s foot, and thus the name pes (foot) anserine (goose).
These three muscles originate in the thigh and hip, but the terminal ends cross the knee joint. Because the tendons cross the knee joint, any increased valgus or medial rotational changes in the knee will in turn place tensile and rotationa stress on the tendons and bursa.
Etiology
Direct trauma, excessive pronation of the feet, and a consequential increased Q-angle are common causes of pes anserine bursitis. Acute trauma to the pes anserine bursa and tendons will cause localized inflammation and swelling, and that should be addressed with rest, elevation, compression, and the application of ice. Adjunctive physiotherapy, including interferential muscle stimulation, ultrasound, and cold laser, may prove helpful. Nutritional supplements to quiet the inflammation and benefit tissue repair should also be considered.
Biomechanical Factors
Some degree of pronation of the feet is normal, especially in the initial weight-bearing stages of the stance gait and while running. The subtalar joint allows this motion in the coronal plane. This motion is normally limited and arrested if the ligaments of the foot ai e healthy and the stabilizing muscles of the foot and leg are performing normally.
The normal anatomy of the knee, with a minimal valgus and Q-angle values, allows for proper biomechanical function (Fig. 2). The knee joint also enjoys a great degree of motion. At first glance, it would appear to have motion in only the sagittal plane, but it actually enjoys three-dimensional motion.3 Three-dimensional range of motion is described as six degrees of freedom.3 Obviously, some motion is greater than others. Nevertheless, the knee does have slight coronal and rotational motion that allows for increases in the valgus stress.
^Custom-made, flexible functional orthotics can reduce the effects of medial knee pain, specifically over the pes anserine bursa, and should be used specifically to care for this malady. J J
Faulty biomechanics of the foot, specifically pronation (Fig. 3), may cause the kinetic chain association between the foot, ankle, knee, and hip to produce symptomatology at the pes anserine bursa. In fact, excessive pronation of the foot almost ensures an increased valgus stress and Q-angle at the knee,
so it is difficult to separate the two findings. In that portion of the gate cycle known as midstance, where the heel and toes are in contact with the ground surface, the tibia and femur are at maximal internal rotation causing potential stress at the medial knee.
An increase in the valgus angulation of the knee and the Q-angle will cause stretching and tension on the tendons of the pes anserine
complex. When the tendons become inflamed, the bursa follows soon thereafter, and a patient can experience pain just below the medial joint line on the proximal tibia.
When this association changes, there is a potential for inflammation and subsequent tendinitis and bursitis. The bursa usually becomes inflamed secondary to contiguous inflammation from the tendons themselves.
Evaluation
To screen for pronation, inspect the barefoot patient in the standing position. Remember that pronation may present unilaterally. Hallmarks of pronation include:
1. Decreased medial longitudinal arches
2. Medially bowed Achilles tendons
3. Foot flare
The increase in valgus angulation and Q-angle of the knee is more readily observed while in front of the patient. Recall that this can be a unilateral or bilateral situation.
Swelling in the knee can be classified as localized (bursal) or generalized (effusion).2 In some cases, the localized edema of the pes anserine bursa may be appreciated upon inspection.
Palpation directly over the pes anserine bursa will usually
illicit a sharp jump from the patient if the tendon complex and adjoining bursa is inflamed. The patient may be unaware of this tenderness. Regardless of the patient’s perception of the inflamed bursa and tendons, the finding of tenderness usually will be present if the condition has been present for some time.
Range of motion of the knee will most likely be normal with some potential pain at extreme flexion. Motor, sensory, and reflex examinations should be within normal limits. The “hinge test” may elicit a pain response.
Tenderness over the medial joint line should not be confused with pes anserine bursitis. This finding usually has a history of significant trauma and may involve sprains or tears of the medial collateral joint ligament or the medial meniscus.2 In the case of pes anserine bursitis, McMurray’s and Apley’s tests should prove negative.2,4 5
Diagnostic studies aie of little benefit in the determination of a diagnosis of pes anserine bursitis. X-ray and MRI will not show any significant changes unless there is a great deal of effusion.6
What to Do
Caring for pes anserine bursitis must include weight-bearing orthotic casting.7 In addition to medial longitudinal support, a pronation wedge is also extremely important. This will allow the calcaneus and forefoot to be repositioned in lateral rotation, which will reduce pronation and medial rotation of the knee joint. Q-angle and valgus stress reduction will follow orthotic casting. Research has shown that
F°°t Levelers’ custom-made functional orthotics (Fig. 4) significantly improve the Q-angle in hyperpronating patients.8
Physiotherapy may be started before or after the feet have been stabilized with functional orthotics. Be aware that if you begin a program of care prior to orthotic usage, then the effects may only be palliative.
Medically, iontophoresis may be performed directly over the pes anserine bursa with a cortisone or similar gel to help reduce inflammation.7
Quadriceps strengthening can begin as soon as the diagnosis is made and if the patient can tolerate the activity. Interferential stimulation, especially over the muscles of the medial compartment of the thigh, can augment tendon strength prior to active rehabilitation.7 Resistance training should target leg extensions, leg lifts, squats, running, walking, cycling, or any other activity that would increase the tonicity of the quadriceps muscles.
Since the primary muscles involved are in the medial and posterior compartments of the thigh, biceps curls should be the core rehab exercises. Foot Levelers’ THERA-CISER exercise
system (Fig. 5) is an excellent, simple, effective choice for at-home strength regimens. The intrinsic muscles of the foot and ankle can be addressed with THERACISER as well.
The talus will often present with excessive anteromedial mobility
and malposition. Changes in the axial skeleton and lower extremities in terms of bone density shifts and positional shifting have been documented following orthotic use.9 Therefore, manual adjustments of the talus and the spine should be performed during the break-in period of the orthotics to reduce adhesions in order to facilitate adaptation to the functional orthotics.
Conclusion
Weight-bearing joints of the lower extremities compose the foundation of the rest of the body. Changes in the support structure of the feet from aging, overuse, daily activities, or athletics can affect the knees and accelerate or precipitate degenerative changes and their precursors.
Doctors of chiropractic need to be cognizant of the widerange effects of pronation of the feet and have protocols for management and care.
References
1. Gray H. Anatomy of the Human Body Philadelphia: Lea and Febiger, 1973:353.
2. Hoppenfeld, S. Physical Examination of the Spine and Extremities. East Norwalk, CT: Appleton-Century-Crofts, 1976:191192.
3. Panjabi M, White A. Biomechanics in the Musculoskeletal System (Isted.). Philadelphia: Churchill Livingstone, 2001:21.
4. Mazion JM. Illustrated Manual of Neurological Reflexes/Signs/ Tests and Orthopedic Signs/Tests/Maneuvers for Office Procedure. Casa Grande, AZ: J.M. Mazion, 1980:218, 231.
5. Haldeman S. Modern Developments in the Principles and Practice of Chiropractic. Norwalk, CT/San Mateo, CA: Appleton and Lange, 1980:294.
6. Firooznia H, Golimbu CN, Rafii M. MRI and CT of the Musculoskeletal System. St. Louis: Mosby-Year Book, 1992:691-696.
7. In house case studies and clinical observations at Dint Chiropractic Center, Laramie, WY, 1995 to present.
8. Kuhn DR, Yochum TR, Cherry AR, Rodgers SS. Immediate changes in the quadriceps femoris angle after insertion of an orthotic device. JManip Physiol Ther. 2002; 25(7):465-470.
9. GreenawaltMH. Spinal Pelvic Stabilization (4th ed.). Roanoke, VA: Foot Leve Iers, Inc. Educational Division, 1990.
Dr. Mark Charrette is a 1980 summa cum laude graduate of Palmer College of Chiropractic. He is a frequent guest speaker at Chiropractic colleges worldwide and has taught over fourteen hundred seminars worldwide on extremity adjusting, biomechanics, and spinal adjusting techniques. Contact info: drmarkcharrelie ftgmail. com