Many questions can be asked about vitamins. A Google search for this term will yield a dizzying number of products, claims, facts, and folly.
Many questions can be asked about vitamins. A Google search for this term will yield a dizzying number of products, claims, facts, and folly.
“Don’t eat anything that your great-great grandmother wouldn’t recognize as food”
—Michael Pollan
Many questions can be asked about vitamins. A Google search for this term will yield a dizzying number of products, claims, facts, and folly.
Four questions for a provider relevant to treating patients are:
1. Why is a vitamin important?
2. How does it work?
3. Where do we get it?
4. How much do we need?
The following will answer these questions about vitamin D.
In the absence of adequate vitamin D, our body’s systems don’t work well. Vitamin D is needed by all cells.
A cell receives a signal for a demand. For the cell to manufacture a given compound to respond, the cell will absorb some 25-hydroxycholecalciferol (vitamin D3) from the bloodstream and activate it to 1,25-dihydroxcholecalciferol. The activated form is a hormone and the key to unlocking the needed information from the intracellular DNA, which, in turn, allows for the proper cellular response.1 This is the basic process for any and all cell types.
In that process, vitamin D is not the cause; it enables the cells’ action. With adequate levels of extracellular vitamin D (typically in the form of 25-hydroxycholecalciferol), the cell can synthesize the active form to properly respond to the stimulus.
All studies in all nations show that the majority of the world’s population has inadequate vitamin D status.2'6 This deficiency will manifest itself differently, depending upon the tissue being stressed.
The list of diseases that coincide with poor vitamin D status is diverse and long. The partial list includes osteoporosis, osteomalacia, rickets, hypertension, cardiac disease, premature births, low birth weight, diabetes, metabolic syndrome, periodontal disease, increased susceptibility to infection, various cancers, multiple sclerosis, influenza, depression, and schizophrenia.7'18
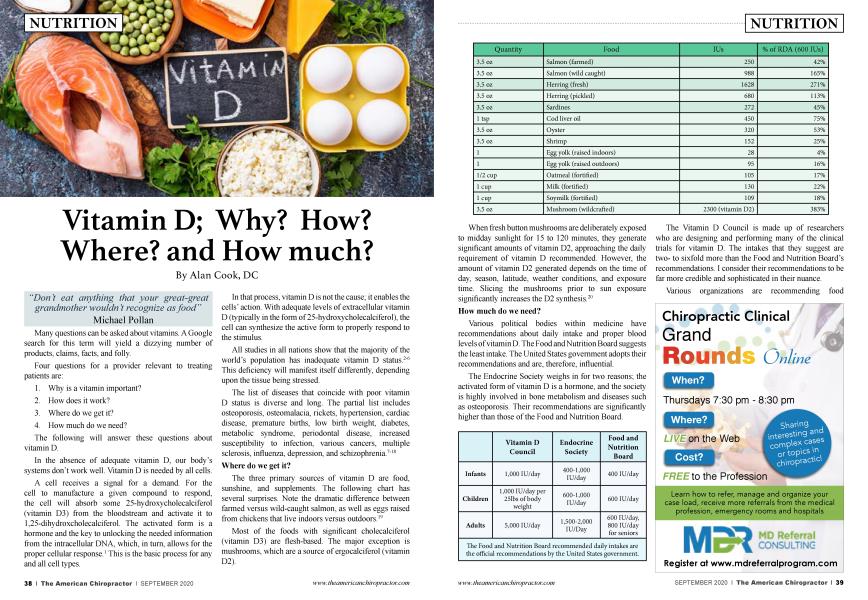
The three primary sources of vitamin D are food, sunshine, and supplements. The following chart has several surprises. Note the dramatic difference between farmed versus wild-caught salmon, as well as eggs raised from chickens that live indoors versus outdoors.19
Most of the foods with significant cholecalciferol (vitamin D3) are flesh-based. The major exception is mushrooms, which are a source of ergocalciferol (vitamin D2).
When fresh button mushrooms are deliberately exposed to midday sunlight for 15 to 120 minutes, they generate significant amounts of vitamin D2, approaching the daily requirement of vitamin D recommended. However, the amount of vitamin D2 generated depends on the time of day, season, latitude, weather conditions, and exposure time. Slicing the mushrooms prior to sun exposure significantly increases the D2 synthesis.20
Various political bodies within medicine have recommendations about daily intake and proper blood levels of vitamin D. The F ood and Nutrition Board suggests the least intake. The United States government adopts their recommendations and are, therefore, influential.
The Endocrine Society weighs in for two reasons; the activated form of vitamin D is a hormone, and the society is highly involved in bone metabolism and diseases such as osteoporosis. Their recommendations are significantly higher than those of the Food and Nutrition Board.
The Vitamin D Council is made up of researchers who are designing and performing many of the clinical trials for vitamin D. The intakes that they suggest are twoto sixfold more than the Food and Nutrition Board’s recommendations. I consider their recommendations to be far more credible and sophisticated in their nuance.
Various organizations are recommending food intakes, but total intake is most important—food plus sunshine plus supplements. These are fine for guidelines, but the blood levels of 25-hydroxycholecalciferol can be measured, which yields an essential finding.
The following are the most common laboratory thresholds used in the United States when measuring 25-hydroxycholecalciferol, the storage form of vitamin D.
25-hydroxycholecalciferol21
Normal >30 ng/ml
Insufficiency 20-30 ng/ml
Deficiency 20 ng/ml
When looking at the blood levels of non-westernized societies (e.g., the Maasai), it’s common to see a level of 60 ng/ml.22 Many vitamin D researchers suggest that optimal levels should be 45-50 ng/ml. These are substantially higher than the 30 ng/ml threshold reported as “normal.”
In the United States, the mean level of 25-hydroxycholecalciferol in white adults is 26 ng/ml. There is some seasonal variability here. The mean level for Hispanics is 21, and it is 16 for African-Americans. All of these are below the 30 ng/ml threshold. This is consistent with findings of deficiency of various ethnic groups across several studies. For example, African Americans have the highest rates of vitamin D deficiency estimated at 82%, Hispanics at 70%, while the US population at large has a reported 42% deficiency.23
There is one other factor adding to the widespread deficiency. As someone’s average weight increases, more vitamin D is needed to combat the “dilution” of this nutrient. Vitamin D is fat-soluble and is incorporated into body fat. Obese patients need two to three times more vitamin D, from whatever source, compared with people at their proper body weight.24
The question of how much to recommend persists. Several vitamin D researchers suggest that adult daily intake should be approximately 4,0006,000 IU from all sources—sunshine, food, and supplements. If someone works and lives indoors and does not eat fish regularly, then a supplement of4,000-6,000 IU/day is reasonable.25
However, if the patient has a blood level of 30 ng/ml, and you are trying to bring them up to 45, you would need an additional 1,500 IUs per day. Serum 25-hydroxycholecalciferol rises by 1 ng/ml for every 100 additional IUs of vitamin D3, whether it’s from sunshine, food, or supplements.25
This formula is an approximation because the patient’s weight is another important variable. The more someone weighs, the more additional D3 is needed. After increasing vitamin D intake, blood levels should be retested 12 to 16 weeks later.
In conclusion, vitamin D is a necessary nutrient that affects multiple organ systems. The notion that vitamin D is only bone-active is antiquated.
Vitamin D can be acquired through the diet—mostly fish, liver, or fortified foods—or via ultraviolet B that strikes skin. Absorption rates, both from the diet or the sun, are highly variable.
Vitamin D has been demonstrated to prevent, treat, or partially treat a growing variety of common diseases.
To know how much vitamin D to prescribe, the best first step is to test for 25-hydroxycholecalciferol. The optimal level is not fully agreed upon, though a substantial number of researchers and expert panels put this at 45-60 ng/ml, which is higher than the current prevailing opinion of 30 ng/ml.
Serum 25-hydroxycholecalciferol levels below 32 ng/ml are not adequate for any body system. Optimal levels can be accomplished with sunshine, dietary intake, or supplements without approaching a level that anyone who is informed would consider toxic. Inputs from all sources combined needed to sustain optimal levels are in the range of 5,000 IU/day. This is far higher than the current adult recommended daily allowance of 600IU.
References
1. Bikle DD. Vitamin D metabolism, mechanism of action, and clinical applications. Chem Biol. 2014;21(3):319-329.
2. Holick M: High prevalence of vitamin D inadequacy and implications for health. Mayo Clinic Proc 2006, 81:353-373.
3. Allain TJ, Dhesi J. Hypovitaminosis D in older adults. Gerontology. 2003;49(5):273-278.
4. O Malley G, Mulkerrin E. Vitamin D insufficiency: a common and treatable problem in the Irish population. Ir J Med Sci. 2011;180:7-13.
5. Arunabh S, Pollack S, Yeh J, Aloia JF. Body fat content and 25-hydroxyvitamin D levels in healthy women. J Clin Endocrinol Metab. 2003;88:157-61.
6. Bandeira F, Griz L, Dreyer P, Eufrazino C, Bandeira C, Freese E. Vitamin D deficiency: a global perspective. Arq Bras Endocrinol Metabol. 2006 Aug;50(4): 640-6.
7. Aranow C. Vitamin D and the immune system. J Investig Med. 2011;59(6):881-886.
8. Zeitz U, Weber K, Soegiarto DW, Wolf E, Balling R, Erben RG. Impaired insulin secretory capaci ty in mice lacking a functional vitamin D receptor. Faseb J. 2003; 17(3) . 509-511.
9. Sigmund CD. Regulation of renin expression and blood pressure by vitamin D(3). J Clin Invest. 2002; 110(2): 155-156.
10. Wagner CL, Greer FR, American Academy of Pediatrics Section on B, American Academy of Pediatrics Committee on N. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008; 122(5): 1142-1152.
11. Jones AN, Hansen KE. Recognizing the musculoskeletal manifestations of vitamin D deficiency. J Musculoskelet Med. 2009;26(10): 389-396.
12. Plotnikoff GA, Quigley JM. Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin Proc. 2003; 78(12): 1463-1470.
13. Al-Khalidi B, Kimball SM, Rotondi MA, Ardern CL Standardized serum 25-hydroxyvitamin D concentrations are inversely associated with cardiometabolic disease in US adults: a cross-sectional analysis of NHANES, 2001-2010. Nutr J. 2017; 16(1): 16.
14. CannellVieth R, Umhau JC, et. al. Epidemic Influenza and Vitamin D. Cambridge University Press (online); 07 Sep 2006.
15. Aloia JF, Li-Ng M. Epidemic Influenza and Vitamin D. Epidemiology and Infection. 2007; 135: 1095-8.
16. Urashima M, Segawa T, Okazaki M, et. al. Randomized Trial of Vitamin D Supplementation to Prevent Seasonal Influenza A in Schoolchildren. Am J ClinNutr. 2010; 91: 1255-60.
17. HoangMTT, DeFina LF, Willis BL, et. al. Association Between Low Serum 25-hydroxyvitamin D and Depression in a Large Sample of Healthy Adults: the Cooper Center Longitudinal Study. Mayo Clinic Pro 1986; 86: 1050-55.
18. Vitamin D and Depressioin: A Systematic Review and Meta-analysis Comparing Studies With and Without Biological Flaws. Nutrients 2014; 6: 1501-18.
19. USDA Food Data Central
20. Keegan RJH, Lu Z, Boqusz JM, Williams JE, Holick MF. Photobiology of vitamin D in mushrooms and its bioavailability in humans. Dermatoendocrinol 2013:5:165-76 +
21. Holick MF. Vitamin D Status: Measurement, Interpretation, and Clinical Application. Ann Epidemiol. 2009; 19:73-8.
22. Luxwolda MF, Kuipers RS, Kema IP, Dijck-Brouwer DA, Muskiet FA. Traditionally living populations in East Africa have a mean serum 25-hydroxyvitamin D concentration of115nmol/1. BrJNutr. 2012; 108:155761.
23. Hanley DA, Davison KS. Vitamin D Insufficiency in North America. JNutr. 2005; 135:332-7.
24. Gallagher JC, Yalamanchili V, Smith EM. The effect of vitamin D supplementation on serum 25(OH)D in thin and obese women. J Steroid Biochem Mol Biol. 2013;136:195-200.
25. Heaney RP. Vitamin D in Health and Disease. Clin J Am Soc Nephrol. 2008;3:1535-4
Alan Cook DC has been in practice since 1989. Currently he is involved in two professional endeavors: 1. Treating patients in a collaborative medical clinic system (Open Door Community Health Center) in Eureka, CA. 2. EasyWebCE; providing chiropractic continuing education in a web-based video format, www.easywebce.com. Reach Dr. Cook at: [email protected] or 707 502-7071 1622 Hyland St. Bayside, CA 95524