Prior to COVID, I did not know that humans have a virome, which is analogous to the microbiome, but consists of viruses instead of bacteria. For context, a standardized male weighing 155 pounds at 20-30 years of age will contain 30 trillion human cells and 39 trillion bacteria cells in the microbiome that weigh about .44 pounds (2). When you consider that there are 100 times more vimses in our bodies than human cells (3), it means we have about 3 quadrillion vimses in our bodies. Therefore, it turns out that about 8% of our genome is represented by viral fragments (3).
Clearly, we are outnumbered by bacteria and vastly outnumbered by vimses, which explains the title of this article. Why is it that we are not perpetually suffering from infection symptoms? This is an important consideration. Anyone reading this article can recall times when they developed cold/flu symptoms without being exposed to other infected individuals. When I was little and going out to play in the snow, my mother would bundle me up because she did not want me to “catch a cold.” Staying wann does not protect one from “catching a vims,” but it does stop the body from suffering a pro-inflammatory stress reaction from excessive cold that disrupts one’s homeostatic and symbiotic relationship with their occupying bacterial and viral populations. Strep throat is a good example of this. Strep pyogenes is part of the natural flora of the respiratory system in many people—however, symptoms emerge only when a stressor is significant enough to disrupt the homeostatic balance.
Save for a novel and virulent infectious agent, it is rarely invading bacteria and viromes that give us symptoms; rather, it is our body that loses its capacity to maintain homeostasis with our occupying bacteria and viromes. We should also realize that we humans share the same species of bacteria and viromes. So, if I happen to be temporarily exposed to someone who is suffering with symptoms reflective of viral homeostasis disruption, I should not be affected so long as my relationship with my virome is symbiotic.
We almost always suffer from this type of ‘self infection’ process.
I witnessed the homeostatic dismption process when I taught in the chiropractic college classroom. The students were fine until the last 2-3 weeks of the tenn, which was when scratchy throats and malaise were much more likely to emerge than any other time during the tenn, as well as more severe “cold” symptoms. Typically, four big lifestyle changes emerge during that time for students. They get less sleep, exercise less, eat less healthy, and experience significantly more mentally stress, which serve as pro-inflammatory stressors that disrupt viral-human cell homeostasis and the immune system overreacts to resident vimses. We could move into an aseptic environment and still suffer these stressors and get viral infection symptoms, because we do not require the presence of additional vimses to develop viral infection symptoms. In reality, we almost always suffer from this type of “self-infection” process.
We should also appreciate that there is no way to avoid “viral infection symptoms” if we inappropriately stress ourselves to an adequate pro-inflammatory degree and disrupt our symbiotic relationship with our virome. This is why we should endeavor to get proper rest and avoid physical and emotional stressors, so that when we do encounter the unavoidable and unexpected stressors of life, we will not suffer from a cumulative event that would otherwise lead to a homeostatic disruption event.
With the above in mind, as early as March 2020, I learned that obese people with hyperglycemia are much more likely to die from a viral infection, which has been known since 1918 during the so-called Spanish flu (it didn’t originate in Spain from Spaniards) and subsequent viral outbreaks (1,2). This opened my eyes to a view of viral infections that I did not previously have. Although I was aware that the pro-inflammatory state of obesity and hyperglycemia functioned to degenerate musculoskeletal and visceral tissues (3), I did not know that they were also promoters of viral infection severity.
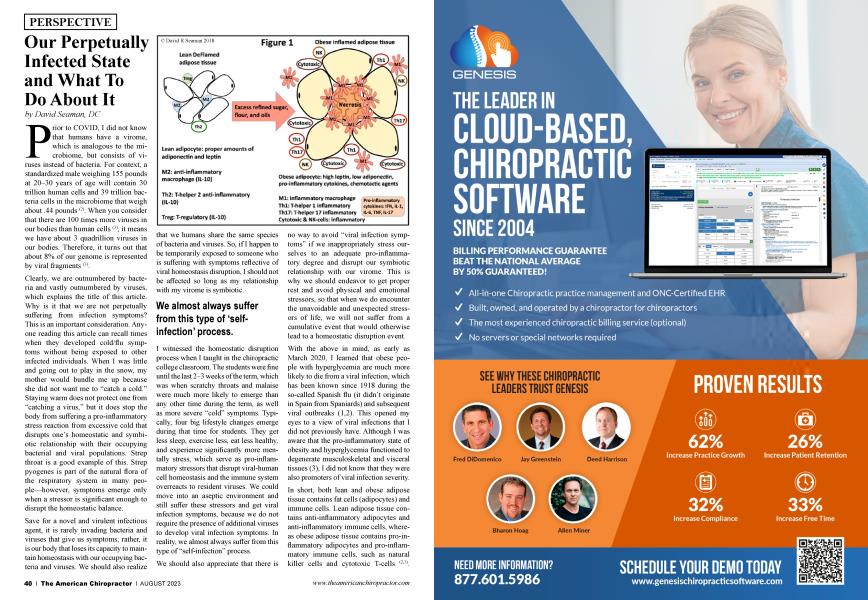
In short, both lean and obese adipose tissue contains fat cells (adipocytes) and immune cells. Lean adipose tissue contains anti-inflammatory adipocytes and anti-inflammatory immune cells, whereas obese adipose tissue contains pro-inflammatory adipocytes and pro-inflammatory immune cells, such as natural killer cells and cytotoxic T-cells (2,3).
These are the immune cells that emerge during a viral infection event and they are perpetually in abundance in the obese state no matter if one is suffering with an active viral infection or not. This is an abnormal immune state and reflects a loss of normal homeostasis, such that obese people are likely to suffer more acute bouts of augmented inflammation compared to lean individuals no matter the stressor. This is why obese people are more likely to get viral infections, stay infected longer, are more contagious, shed more viruses, and produce more viral mutations with increased virulence compared to lean people (4). For these reasons, obese people are considered to be super-spreaders of viral infections(5). Rather than having a symbiotic and homeostatic relationship with their virome, the immune systems of obese people have a relationship that is more adversarial and pro-inflammatory, which is unhealthy for the obese individual and those around them.
Although obesity and hyperglycemia commonly coexist, I should mention that hyperglycemia directly impacts how one handles a viral infection. Virally infected cells are supposed to react by inserting recognition markers on their cell membranes so they can be eliminated by phagocytes. This process occurs less effectively in the virally infected cells of obese individuals (1), which is made worse by hyperglycemia because it inhibits the activity of phagocytes (6>.
Prior to COVID, I did not know how obesity and hyperglycemia influenced the relationship among human cells, bacteria, and viruses. Although I did know that human cells were outnumbered by bacteria, I did not know that viruses outnumber human cells by 100. This information caused me to realize that the human body essentially lives in a perpetually infected state that can be symbiotic or pro-inflammatory. To maintain a proper symbiotic relationship with our microbiome and virome, we absolutely need to avoid obesity and hyperglycemia, which means we need to get adequate sleep, stay physically active, avoid excess mental/emotional stressors, maintain an appropriate body weight, and eat healthy whole foods. The non-inflammatory state created by these healthy lifestyle choices can be further augmented by taking various nutritional supplements, such as vitamins D and C, zinc, polyphenols, probiotics, magnesium, and omega-3 fatty acids (2>3).
David Seaman, DC, is consultant for Anabolic Laboratories and has designed several nutritional supplements. He has authored many articles on the topic of diet, inflammation, and pain. His most recent book written for laypeople is entitled The DeFlame Diet. He posts regular DeFlame nutrition updates at DeFlame Nutrition on YouTube and Facebook..
References
1.Luzi L, Radaelli MG. Influenza and obesity: its odd relationship and the lessons for the COVID-19 pandemic. Acta Diabetologica. 2002;57:759-64.
2.Seaman DR. The DeFlame Diet for Immune Health. Wilmington (NC): Shadow Panther Press, 2020.
3.Seaman DR. The DeFlame Diet to Stop Your Joints, Muscles, and Bones from Rotting. Wilmington (NC): Shadow Panther Press, 2020.
4.Luzi L, Radaelli MG. Influenza and obesity: its odd relationship and the lessons for the COVID-19 pandemic. Acta Diabetologica. 2002;57:759-64.
5.Edwards DA, et al. Exhaled aerosol increases with COVID-19 infection, age, and obesity. Proc Nat Acad Sci. 2021; 118(8).e2021830118.
6.Lecube A, et al. Phagocytic activity is impaired in type 2 diabetes mellitus and increases after metabolic improvement. PLoS ONE 6(8) e23366. doi:10.1371/joumal.pone.0023366.