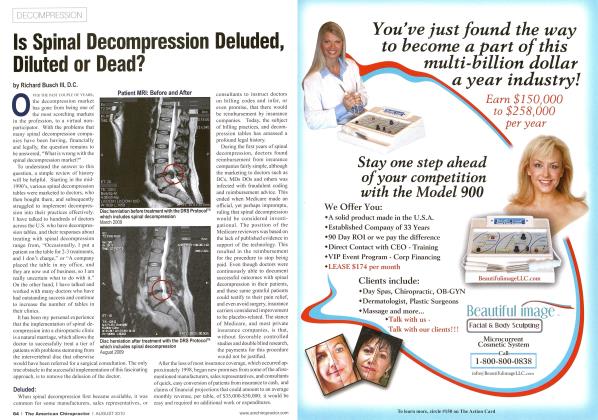
Over the last 25 years, I have been treating a tier of patients that many chiropractors would never think of accepting as patients, or they would immediately refer them to a surgeon. However, I have successfully treated thousands of this tier of patient with nonsurgical spinal decompression. Most suffered from severe and chronic disc-related conditions, including failed back surgery syndrome (FBSS). Many patients had been evaluated by a surgeon, and surgery was recommended. Most of the other patients had known about the possibility of less-than-stellar outcomes from back surgery and wanted to take a more conservative direction of care.
I have dedicated my life to helping patients avoid needless surgeries and unnecessary medications. Many of the patients I have treated have been through the “back and neck pain pipeline,” which refers to previous less successful treatments and includes chiropractic care, physical therapy, multiple epidurals, spinal surgeries, and spinal fusions.
As a chiropractor, I believe in treating patients with chiropractic care. However, for more involved cases, additional tools are needed to achieve maximum improvement. For this reason, in 1997 I developed a successful nonsurgical decompression protocol that enabled me to treat a tier, or type, of patient that many chiropractors cannot or do not have the confidence to treat. That is the DRS Protocol™, with nonsurgical spinal decompression as the centerpiece. This protocol can help severe and chronic disc-condition patients and (FBSS) patients.
During future issues of the American Chiropractor, I will be contributing a column to discuss some of the more complicated conditions I treat and how to treat them successfully.
This first article will focus on treating patients with FBSS, many of whom have previously had discectomies, foraminotomies, and laminectomies. In a future article, I will discuss the treatment of some other complicated situations like spinal fusion surgery patients.
There are conditions that can complicate FBSS cases, which I will also be discussing in future articles. These conditions include but are not limited to: recurrent disc herniation, adjacent segmental disease, epidural fibrosis or scar tissue, radiculopathies and paresthesia following surgery, nerve root irritation and many others.
When spinal decompression is performed correctly, it can significantly help these patients. I have successfully treated thousands of patients who have suffered from these complications. Patients are frequently reevaluated and at times treatment may also require additional therapies to maximize outcomes.
In working with complicated cases, I follow the normal office procedures. There must always be an in-depth case history. Case histories are necessary for any condition, as we have learned 80% of a diagnosis comes from the case history. A detailed case history is essential for FBSS patients because of the complicated nature of their condition.
A thorough physical exam that includes orthopedic, neurologic, and chiropractic examinations is required, as are X-rays, MRIs and CTs when indicated. We leave no stone unturned, as the goal is to achieve the best possible results.
Some indicators we are looking for from patients’ histories include what other treatments they have had and how successful the treatments were. The answers to these questions are a strong predictor of how well the patient is going to respond to treatment. As an example, if a patient has responded to epidurals, for even a short period, this is a strong indication that the patient will respond favorably to spinal decompression.
In the case history, note how many back surgeries have been performed, surgery dates, other related treatments, and how the patient responded to each.
The primary rule for treating surgical patients is “no treatment” for at least six weeks post-surgery and up to eight months for some surgeries. An additional challenge is scar tissue following surgery. Scar tissue is contractile and can, over time, put additional pressure on the spinal nerves as they exit the spinal canal and or spinal cord.
When treating post-surgical patients with nonsurgical spinal decompression, I generally use a lower treatment parameter setting, or less force, than usual. In my 25 years of experience, the concept of “less is more” is much like the use of the Activator Method. It is important to remember that increasing the force may have the opposite effect of creating more pain, muscle guarding, and mobility concerns.
In determining the lumbar spine parameter calculation for spinal decompression, I use the following calculations: 50% body weight minus 20 pounds for the starting parameter and 50% body weight plus 20 pounds for the top parameter setting. The starting parameter is the weight of force applied to the patient when starting care. The top parameter is the maximum force applied to the patient during treatment. Although I calculate the top parameter setting when beginning treatment, most of my patients never reach the top parameter setting.
Decompression begins at different forces for different individuals. Since each patient is an individual case, I look at the different characteristics of each patient. I determine the parameters based on the patient’s overall physical makeup. Lower muscle mass generally means less weight. I may begin treatment as low as 50 pounds of force. The opposite is also true, the greater the muscle mass, the higher the force.
Next, I determine the level of disc involvement and the angle necessary to target the involved disc level. If the level of disc involvement is L5/S1, and the L4 disc is neurologically involved, I alter the angle of force by adding 5 degrees. Instead of applying force at a normal 5-degree angle, I add 5 degrees to the angle, so the angle is now 10 degrees. During treatment, ask the patient about comfort. The angle may be adjusted according to the patient’s comfort.
There is no question that nonsurgical spinal decompression is a powerful treatment for severe and chronic disc-related conditions. I believe nonsurgical spinal decompression is one of the most effective treatments a chiropractor can employ to help patients avoid back and neck surgery. Many FBSS patients can also be treated successfully with spinal decompression. Just keep these concepts in mind: complete history, thorough exam, and the appropriate imaging studies. Remember, less is more, and carefully determine the proper force and angle. Add other therapies as needed for more complicated conditions and better results.
I look forward to discussing other complicated conditions in the next article.
Dr. Richard E. Busch III has been in private practice in Fort Wayne, IN since 1996. He has built one of the largest spinal decompression and cash practices in the world. Dr. Busch has also trained many chiropractors and medical doctors in prepaid case fee cash practice. For more information go to Cashmasterpractice.com: 5005 Riviera Ct„ Fort Wayne, IN. 888-471-4090 or [email protected].
References
1. JPhys Ther Sci. 2015 Feb; 27(2): 481-483. Published online 2015 Feb 17. doi: 10.1589/ jpts. 27.481
2. Amjad et al. BMC Musculoskeletal Disorders (2022) 23:255. https://doi.org/10.1186/ si2891-022-05196-x
Catch this interview and many more TAC TIC Talks by scanning the QR code or visiting this link: tacadmin.qrd.by/TACTicTalk