SPORTS-RELATED CONCUSSIONS (SRC) HAVE HISTORICALLY BEEN MISUNDERSTOOD. From antiquated management recommendations, outdated ideas related to pathophysiology, and a hesitation to implement updated evidence, sports clinicians, coaches, parents, and sports teams often report a lack of clarity regarding the management of SRCs.
The Amsterdam 2022 International Consensus Statement1 highlighted clear and practical guidelines to frame how we should approach the management of SRC. The guidelines reinforce that recovery is not merely about waiting for symptoms to fade. It requires a proactive strategy that addresses an athlete’s unique neurophysiological, autonomic, and biomechanical impairments that can arise following SRC.
To illustrate these principles in practice, we’ll follow the case of Jack, a 16-year-old high school hockey player who sustained a concussion during a game. Using Jack’s case as an example, we’ll explore how the latest research, clinical tools, and the integration of sports chiropractic care can optimize SRC management.
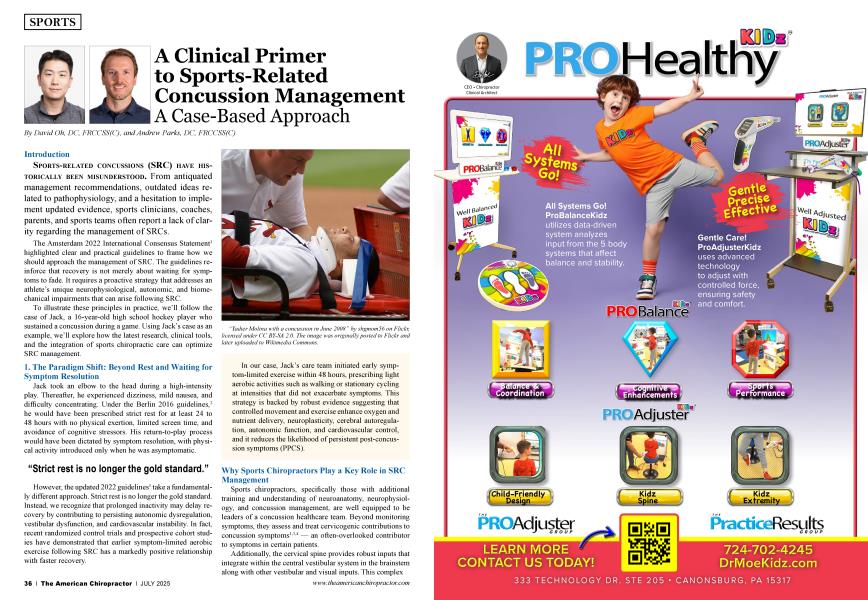
Jack took an elbow to the head during a high-intensity play. Thereafter, he experienced dizziness, mild nausea, and difficulty concentrating. Under the Berlin 2016 guidelines,2 he would have been prescribed strict rest for at least 24 to 48 hours with no physical exertion, limited screen time, and avoidance of cognitive stressors. His return-to-play process would have been dictated by symptom resolution, with physical activity introduced only when he was asymptomatic.
“Strict rest is no longer the gold standard.”
However, the updated 2022 guidelines1 take a fundamentally different approach. Strict rest is no longer the gold standard. Instead, we recognize that prolonged inactivity may delay recovery by contributing to persisting autonomic dysregulation, vestibular dysfunction, and cardiovascular instability. In fact, recent randomized control trials and prospective cohort studies have demonstrated that earlier symptom-limited aerobic exercise following SRC has a markedly positive relationship with faster recovery.
In our case, Jack’s care team initiated early symptom-limited exercise within 48 hours, prescribing light aerobic activities such as walking or stationary cycling at intensities that did not exacerbate symptoms. This strategy is backed by robust evidence suggesting that controlled movement and exercise enhance oxygen and nutrient delivery, neuroplasticity, cerebral autoregulation, autonomic function, and cardiovascular control, and it reduces the likelihood of persistent post-concussion symptoms (PPCS).
 “Yadier Molina with a concussion in June 2008" by shgmom56 on Flickr, licensed under CC BY-SA 2.0. The image was originally posted to Flickr and later uploaded to Wikimedia Commons.
“Yadier Molina with a concussion in June 2008" by shgmom56 on Flickr, licensed under CC BY-SA 2.0. The image was originally posted to Flickr and later uploaded to Wikimedia Commons.
Sports chiropractors, specifically those with additional training and understanding of neuroanatomy, neurophysiology, and concussion management, are well equipped to be leaders of a concussion healthcare team. Beyond monitoring symptoms, they assess and treat cervicogenic contributions to concussion symptoms1’3,4 — an often-overlooked contributor to symptoms in certain patients.
Additionally, the cervical spine provides robust inputs that integrate within the central vestibular system in the brainstem along with other vestibular and visual inputs. This complex but often underappreciated integration is the foundation that allows us to move and navigate in a dynamic and ever-changing physical environment when we are healthy.
Aberrant inputs from one or more of these systems may result in a sensory mismatch, which can drive feelings of dissociation, unsteadiness, visual disturbances, nausea, persistent neck pain, and emotional dysregulation. Additionally, this central vestibular integration is tightly intertwined with autonomic nervous system reflexes through vestibulo-sympathetic pathways.
These reflexes mediate blood distribution to the cerebrum based on sensory feedback of where the body and head are in space. Dysregulation of these reflexes may lead to hypoperfusion of the cerebrum, resulting in symptoms including but not limited to lightheadedness, visual changes, dizziness, headaches, and exercise intolerance. Therefore, assessment and rehabilitation should aim at identifying and actively treating these sensory and integrative errors through rehabilitation.
A case series by Gennann et al. (2020)3 highlights the effectiveness of multi-modal interventions, including:
• Manual therapy for the cervical spine to address somatosensory dysfunction and concomitant musculoskeletal pain.
• Vestibulo-ocular rehabilitation to optimize head and eye coordination and oculomotor control.
• Graduated aerobic exercise exposure to stabilize autonomic control of blood pressure and heart rate while facilitating oxygen and nutrient delivery.
• Deep neck flexor exercises to improve cervical stability, cervical proprioceptive function, and reduce headache intensity.
It is essential to note that the mechanisms of such dysregulation may be different between injuries and in different age cohorts. Thus, objective biometric assessment of autonomic nervous system function via HR, HRV, pupillometry, and exercise measurements are valuable to monitor recovery trajectories and aid in rehabilitation prescription.
A recent systematic review by Parks et al. (2023)5 synthesizes the existing literature on autonomic nervous system dysfunction in pediatric SRC. There is also emerging evidence to suggest value in implementing objective oculomotor testing via video-oculography (VOG) or other eye-tracking devices to detect subtle disturbances in the smooth pursuit, saccade, optokinetic, and visual systems.
A 2025 study by Oh et al. (BMJ Open Sport & Exercise Medicine)6 underscores a crucial finding: timing of care is critical. Athletes who sought care within seven days of injury recovered an average of four days faster than those who delayed treatment (18 versus 22 days median recovery time).
Jack’s parents were initially unsure whether immediate care was necessary, but they decided to take him to a sports chiropractor within 48 hours of injury. Here’s why that decision mattered:
• Timely autonomic assessment allowed for targeted interventions and graded exercise therapy, specifically catered to Jack’s findings.
• Faster integration of cervical and vestibular rehabilitation prevented compounding dysfunctions via aberrant sensory inputs from respective systems.
“A very important point is that the implementation of oculomotor and vestibular rehabilitation is highly specific to the individual and their specific findings.”
Jack reported neck pain and dizziness, which may suggest cervical, vestibular, autonomic, or visual components to his symptoms. His sports chiropractor integrated modalities to assess and target each of these neurological domains where appropriate. Some strategies included sub-symptoms exercise, manual therapy and joint repositioning training of the cervical spine, deep neck flexor training, and oculomotor rehabilitation into his treatment plan.
A very important point is that the implementation of oculomotor and vestibular rehabilitation is highly specific to the individual and their specific findings. Many intricate and overlapping systems connect the cerebellum, cortex, and brainstem to drive the control of eye movement, including eye movement latency, velocity, and accuracy during smooth pursuits, saccades, and combined head-eye movement. Using a generalist approach and applying the same exercises for each patient is not recommended because it may make an individual more symptomatic and is nonspecific to their individual injury or neurology.
Sideline assessments like the SCAT6 are excellent for acute concussion screening, but for in-office evaluations, chiropractors benefit from a more structured tool — the Sport Concussion Office Assessment Tool 6 (SCOAT6)1 designed for ongoing monitoring, ideally used in an office setting.
When Jack arrived at his chiropractor’s office, his SCOAT6 assessment included:
• Symptom burden tracking to monitor changes over time.
• Vestibular-ocular testing to identify visual motion sensitivity or dysfunction.
• Cervical spine examination to assess range of motion and segmental dysfunction.
• Autonomic function assessment, including HRV and orthostatic intolerance screening.
It’s important to note that the SCOAT6 is an incredibly accessible tool that is easy to implement for most practitioners. It does not rely on any advanced diagnostic technology and is easily applied at the bedside with minimal equipment.
That said, the use of the SCOAT6 does not discount the potential for more advanced testing if indicated and required in certain cases. There may be large examiner variability with the techniques and subjective interpretation of a bedside evaluation of oculomotor control and vestibular function.
“...can we treat something to the best of our ability if we do not measure it and deeply understand the breadth and depth of it?”
More objective and reproducible measures, such as vestibulo-oculography (VOG) and posturography, may provide more accurate data and allow for more valid visit-to-visit comparisons throughout recovery. The use of such equipment is largely reserved for practitioners who solely treat traumatic brain injury and other neurological disorders.
In this case, Jack’s chiropractor gained data from the SCOAT6 to refine his rehab plan. The tool ensured that Jack’s treatment evolved dynamically, adapting to his progress rather than relying on outdated stepwise and algorithmic recovery models. No advanced diagnostic equipment was used in the evaluation of this case.
The Amsterdam 2022 guidelines,1 alongside the SCOAT6, help provide clarity and individualized context in the management of athletes with SRC. Sports chiropractors have an important role to play as neuromusculoskeletal experts to promote earlier assessment, diagnosis, and individualized rehabilitation/treatment to help athletes return safely to sport.
However, with each new concussion case we attend to, we must pause, reflect, and ask ourselves the following question with humility: can we treat something to the best of our ability if we do not measure it and deeply understand the breadth and depth of it?
SRC is a complex injury, and it is important to recognize when it is appropriate to refer to a colleague or medical specialist for advanced objective biometric testing or comanagement.
Dr. Andrew Parks is sports specialist chiropractor and fellow of the Royal College of Chiropractic Sports Sciences (RCCSS) Canada. He practices in Ontario Canada and his past research has been published in peer-reviewed journals. His practice population includes those with concussion or other neurological disorders, and he also works as part of an interdisciplinary team programming neurological and physical performance programs for healthy individuals.
Dr. David Oh is a Fellow of the RCCSS(C) with a clinical focus on performance-based rehabilitation and sustainable athleticism. He has worked with a diverse range of athletes at the national and international stage. He is also a clinical instructor and researcher at CMCC and an ECHO Concussion Hub Expert.
1. Patricios JS, Schneider KJ, Dvorak J, Ahmed OH, Blauwet C, Cantu RC, Davis GA, Echemendia RJ, Makdissi M, McNamee M, Broglio S, Emery CA, Feddermann-Demont N, Fuller GW, Giza CC, Guskiewicz KM, Hainline B, Iverson GE, Kutcher JS, Leddy JJ, Maddocks D, Manley G, McCrea M, Purcell EK, Putukian M, Sato H, Tuominen MP, Turner M, Yeates KO, Herring SA, Meeuwisse W. Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport-Amsterdam, October 2022. Br J Sports Med. 2023 Jun;57(ll):695-711. doi: 10.1136/ bjsports-2023-106898. PMID: 37316210.
2. McCrory P, Meeuwisse W, Dvorak J, Aubry M, Bailes J, Broglio S, Cantu RC, Cassidy D, Echemendia RJ, Castellani RJ, Davis GA, Ellenbogen R, Emery C, Engebretsen L, Feddermann-Demont N, Giza CC, Guskiewicz KM, Herring S, Iverson GE, Johnston KM, Kissick J, Kutcher J, Leddy JJ, Maddocks D, Makdissi M, Manley GT, McCrea M, Meehan WP, Nagahiro S, Patricios J, Putukian M, Schneider KJ, Sills A, Tator CH, Turner M, Vos PE. Consensus statement on concussion in sport-the 5th International Conference on Concussion in Sport held in Berlin, October 2016. Br J Sports Med. 2017 Jun;51(ll):838-847. doi: 10.1136/bjsports-2017-097699. Epub 2017 Apr 26. PMID: 28446457.
3. Germann D, Marshall C, Kazemi M. Multi-modal management of sport and non-sport related concussion by chiropractic sports specialists: a case series. J Can Chiropr Assoc. 2020 Dec;64(3):214-226. PMID: 33487643; PMCID: PMC7815178.
4. Cancelliere C, Howitt S, Halowski T, Jacobs C, Da Roza M, Wright D, Connell G, Yu H. Expanding concussion care in Canada: the role of chiropractors and policy implications. J Can Chiropr Assoc. 2024 Aug;68(2): 86-97. PMID: 39318838; PMCID: PMC11418793.
5. Parks A, Hogg-Johnson S. Autonomic nervous system dysfunction in pediatric sport-related concussion: a systematic review. J Can Chiropr Assoc. 2023 Dec;67(3):246-268. PMID: 38283159; PMCID: PMC10814701.
6. Oh DY, Germann D, Cancelliere C, Kazemi M, Marshall C, Hogg-Johnson S. Association of early versus late care seeking for sport-related concussion in adolescent athletes in Canada: a historical cohort study. BMJOpen SportExercMed. 2025 Feb8;ll(l):e002241. doi: 10.1136/bmjsem-2024-002241. PMID: 39931637; PMCID: PMC 11808907.
Disclosures:
The authors used AI technologies (ChatGPT) to proofread and suggest improvements in wording and grammar for this manuscript. All sections were initially written by the human authors and revised by them after artificial intelligence assistance.