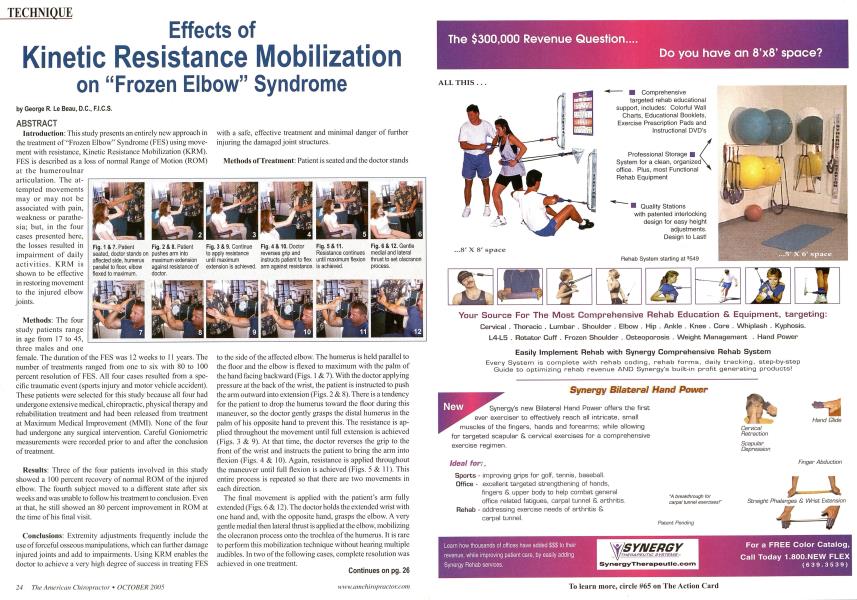
ABSTRACT Introduction: This study presents an entirely new approach in the treatment of "Frozen Elbow" Syndrome (FES) using movement with resistance, Kinetic Resistance Mobilization (KRM). FES is described as a loss of nomial Range of Motion (ROM) at the humcroulnar articulation. The attempted movements may or may not be associated with pain, weakness or parathe-sia; but, in the four cases presented here, the losses resulted in impairment of daily activities. KRM is shown to be effective in restoring movement to the injured elbow joints. Methods: The four study patients range in age from 17 to 45, three males and one female. The duration of the FES was 12 weeks to 11 years. The number of treatments ranged from one to six with 80 to 100 percent resolution of FES. All four cases resulted from a specific traumatic event (sports injury and motor vehicle accident). These patients were selected for this study because all four had undergone extensive medical, chiropractic, physical therapy and rehabilitation treatment and had been released from treatment at Maximum Medical Improvement (MMI). None of the four had undergone any surgical intervention. Careful Goniomctric measurements were recorded prior to and after the conclusion of treatment. Results: Three of the four patients involved in this study showed a 100 percent recovery of normal ROM of the injured elbow. The fourth subject moved to a different state after six weeks and was unable to follow his treatment to conclusion. Even at that, he still showed an 80 percent improvement in ROM at the time of his final visit. Conclusions: Extremity adjustments frequently include the use of forceful osseous manipulations, which can further damage injured joints and add to impairments. Using K.RM enables the doctor to achieve a very high degree of success in treating FES with a safe, effective treatment and minimal danger of further injuring the damaged joint structures. Methods of Treatment: Patient is seated and the doctor stands to the side of the affected elbow. The humerus is held parallel to the floor and the elbow is flexed to maximum with the palm of the hand facing backward (Figs. 1 & 7). With the doctor applying pressure at the back of the wrist, the patient is instructed to push the arm outward into extension (Figs. 2 & 8). There is a tendency for the patient to drop the humerus toward the floor during this maneuver, so the doctor gently grasps the distal humerus in the palm of his opposite hand to prevent this. The resistance is applied throughout the movement until full extension is achieved (Figs. 3 & 9). At that time, the doctor reverses the grip to the front of the wrist and instmcts the patient to bring the ami into flexion (Figs. 4 & 10). Again, resistance is applied throughout the maneuver until full flexion is achieved (Figs. 5 & 11). This entire process is repeated so that there are two movements in each direction. The final movement is applied with the patient's ami fully extended (Figs. 6 & 12). The doctor holds the extended wrist with one hand and, with the opposite hand, grasps the elbow. A very gentle medial then lateral thnist is applied at the elbow, mobilizing the olecranon process onto the trochlca of the humerus. It is rare to perform this mobilization technique without hearing multiple audiblcs. In two of the following cases, complete resolution was achieved in one treatment. Continues on pg. 26 Case Presentations 1. A 17-ycar-old female judo athlete was thrown to the mat during eompetition and landed with her left arm extended. The force of impact fractured the head of the radius and dislocated the radius and ulna at the olecranon process and distal humcrus (Fig. 13, X-Ray). Closed reduction of the dislocation was performed at the emergency room, along with soft casting of the radial head fracture. Physical therapy and rehabilitative exercises were started at four weeks and patient was released to MM I at 11 weeks. She presented for treatment at my office at 12 weeks post injury, with lull flexion, but 50 percent loss of extension at 45 degrees of movement, and moderate pain during movement. After examination and measurements, K.RM was applied and, during the second extension maneuver, a loud audible was heard, whereupon the patient was able to extend her ami fully with no pain. Follow up was performed at six weeks after the treatment and the patient was 100 percent. 2. A 28-year-old male states he suffered an elbow injury while pitching in a high school baseball game. He states his coach kept him in the game even after his having thrown more than 120 pitches. On his final pitch, he felt a snap in his elbow and could no longer bend his ami past 60 degrees of flexion. After several weeks of intensive therapy, he was told that he would require surgery to correct his FES and rcsultinn loss of ROM. He refused the surgery, gave up baseball and went on to college. At the time of his treatment, he stated his major complaint was he could not touch his head (bmsh his hair or wash his head or neck) with his right hand. KRM was applied; there was a very loud audible and, immediately, he was able to bring his hand to the back of his neck. He had suffered with this impairment for 11 years! 3. A 45-year-old medically retired police officer was injured in a motor vehicle accident when a drunk driver "T-Boned" him at his driver's door. Fire Rescue EMT's used the "jaws of life" to pry his door open. During the rescue operation, the lower blade of the "jaws of life" came into contact with the officer's left elbow, fracturing both the proximal radius and ulna. After extensive medical, physical therapy and rehabilitation treatment for more than a year, he was released to MMI and medically retired with a permanent impairment of 30 percent loss of flexion at 60 degrees and 50 percent loss of extension at 45 degrees. When I treated the patient for the first time, he was seven years post injury. I treated him with KRM once a week for six weeks. During that time, he had a dramatic improvement in his ROM; but, after the sixth treatment, he informed me that he was in the process of moving and was unable to complete treatment. Final measurements were taken at that time to document his progress. He showed a 20 percent improvement in flexion at 80 degrees (up from 60 degrees) and a 25 percent improvement of extension to 60 degrees (up from 45 degrees). I designed a set of rehabilitative exercises for this patient and followed up with him by phone for several months. The exercises consisted of using surgical tubing resistance bands to assist with KRM (Figs. 15 & 16). 4. A 30-year-old male fell while riding a mountain bike. He landed with his right arm extended and fractured his proximal radius. He was treated with immobilization (soft cast) and wore a sling. He was released with no further treatment after eight weeks. The patient was treated with KRM two years after his injury. Although his radius was completely healed, he had pain on movement and his residual loss of extension was measured at 55 degrees. During the fourth treatment with K.RM, there was a significant audible and the patient was able to fully extend his ann for the first time in two years. Results The dramatic results reported here suggest a completely new approach to extremity manipulation with possible future application to spinal adjustments. Treatment ranging from one to six weeks resulted in a total average improvement of 73 percent, with three of the patients achieving complete resolution of their symptoms and 100 percent improvement in their ROM (Fig. 14, Bar Chart). Application of K.RM can become a safe, yet effective, alternative to forced osseous manipulations, which have the potential of adding further trauma to the involved joint. Conclusions Certainly, further clinical trials under a more structured environment arc advised and recommended. In addition to FES, I am currently in the process of developing and implementing KRM in the treatment of other extremity disorders, specifically the shoulder, wrist (carpal tunnel syndrome), hip (fixated femur head), knee (fibula subluxation, tibial plateau rotation and patella subluxation), and ankle-foot syndromes (tarsal tunnel, foot drop and plantar fasciitis). Interested parties are encouraged to contact the author for further infonnation on KRM as well as joint venture (no pun intended) participation in future clinical trials. _ February 12-15.2006 PANAMA ^ Speaker At Dr. George Le Beau. FIL'S, has been in private practice 33 years. He was US Olympic Judo Team doctor for 10 years and has taught more than 300 seminars on treatment of sports injuries and extremity technique. He is an Associate Professor at Cleveland Chiropractic College of Los Angeles. He can be reached at Dr-George(ipsbcglobal.nei.WBM Fig. 1 & 7. Patient seated, doctor stands on affected side, humerus parallel to floor, elbow flexed to maximum. Fig. 2 & 8. Patient pushes arm into maximum extension against resistance of doctor. Fig. 3 & 9. Continue to apply resistance until maximum extension is achieved. Fig. 4 & 10. Doctor reverses grip and instructs patient to flex arm against resistance. Fig. 5 & 11. Resistance continues until maximum flexion is achieved. Fig. 6 & 12. Gentle medial and lateral thrust to set olacranon process. Fig. 13. X-Ray, complete dislocation of proximal radius and ulna with fracture of radial head. Fig. 14. Initial measurements of ROM (blue bar), subsequent measurements at conclusion of treatment (red bar). Fig. 15 & 16. Rehabilitative Exercises using surgical tubing for resistance during flexion & extension.