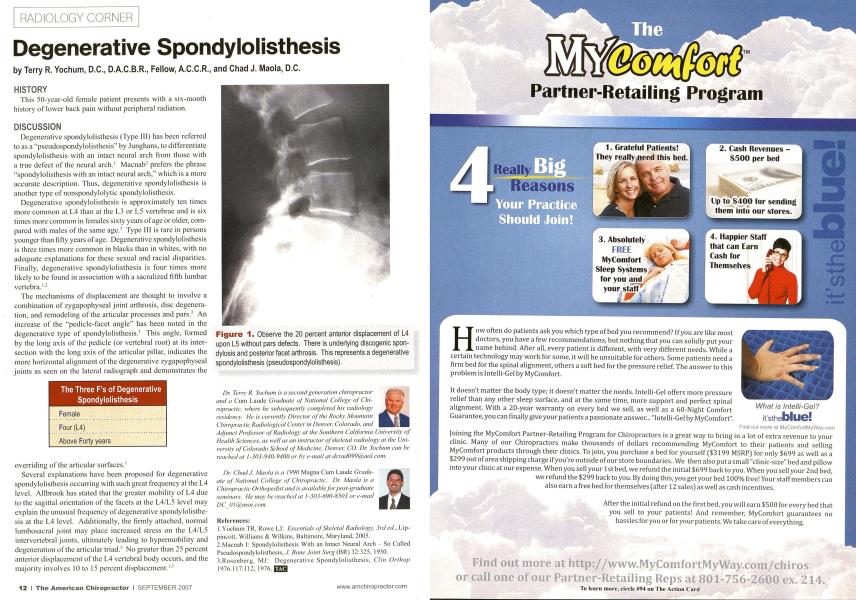
HISTORY This 50-ycar-old female patient presents with a six-month history of lower back pain without peripheral radiation. DISCUSSION Degenerative spondylolisthesis (Type III) has been referred to as a "pseudospondylolisthesis" by Junghans, to differentiate spondylolisthesis with an intact neural arch from those with a true defect of the neural arch.1 Macnab2 prefers the phrase "spondylolisthesis with an intact neural arch," which is a more accurate description. Thus, degenerative spondylolisthesis is another type of nonspondylolytic spondylolisthesis. Degenerative spondylolisthesis is approximately ten times more common at L4 than at the L3 or L5 vertebrae and is six times more common in females sixty years of age or older, compared with males of the same age.1 Type III is rare in persons younger than fifty years of age. Degenerative spondylolisthesis is three times more common in blacks than in whites, with no adequate explanations for these sexual and racial disparities. Finally, degenerative spondylolisthesis is four times more likely to be found in association with a sacralized fifth lumbar vertebra.1-2 The mechanisms of displacement are thought to involve a combination of zygapophyseal joint arthrosis, disc degeneration, and remodeling of the articular processes and pars.2 An increase of the "pedicle-facet angle" has been noted in the degenerative type of spondylolisthesis.1 This angle, formed by the long axis of the pedicle (or vertebral root) at its intersection with the long axis of the articular pillar, indicates the more horizontal alignment of the degenerative zygapophyseal joints as seen on the lateral radiograph and demonstrates the The Three F's of Degenerative Spondylolisthesis Female Four (L4) Above Forty years overriding of the articular surfaces.1 Several explanations have been proposed for degenerative spondylolisthesis occurring with such great frequency at the L4 level. Allbrook has stated that the greater mobility of L4 due to the sagittal orientation of the facets at the L4/L5 level may explain the unusual frequency of degenerative spondylolisthesis at the L4 level. Additionally, the firmly attached, normal lumbosaeral joint may place increased stress on the L4/L5 intervcitebral joints, ultimately leading to hypermobility and degeneration of the articular triad.' No greater than 25 percent anterior displacement of the L4 vertebral body occurs, and the majority involves 10 to 15 percent displacement.1' Dr. Terry R. Yochnm ix a .secondgeneration chiropractor and a Cum Laudc Graduate of National College of Chiropractic, where he snhsei/iienlly completed his radiology residency. He is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, ax well ax an inslriiclor of skeletal radiology at the University of Colorado School of Medicine, Denver, CO. Dr. Yochmn can he reached at 1-303-940-9400 or hv e-mail at dcrad099(i0ciol.coin. Dr. Chad.I. Maola is a 1990 Magna Cum Laude Graduate of National College of Chiropractic. Dr. Maola is a Chiropractic Orthopedist and is available for post-graduate seminars. He may he reached at I-303-690-H503 or e-mail DC_OI(@insn. com. References: I .Yocluim TR, Rowe L.I: Essentials of Skeletal Radiology, 3rd eel.. Lip- pincutt. Williams & Wilkins. Baltimore. Maryland. 2005. 2.Mucnab I: Spondylolisthcsis With an Intact Neural Arch - So Called Pscudospondylolisthcsis.7. Bone Joint Surg (BR) 32:325, 1950. 3.Rosenberg. MJ: Degenerative Spondylolisthesis. Clin Orthop 1976.117:112,1976.1 Figure 1. Observe the 20 percent anterior displacement of L4 upon L5 without pars defects. There is underlying discogenic spondylosis and posterior facet arthrosis. This represents a degenerative spondylolisthesis (pseudospondylolisthesis).