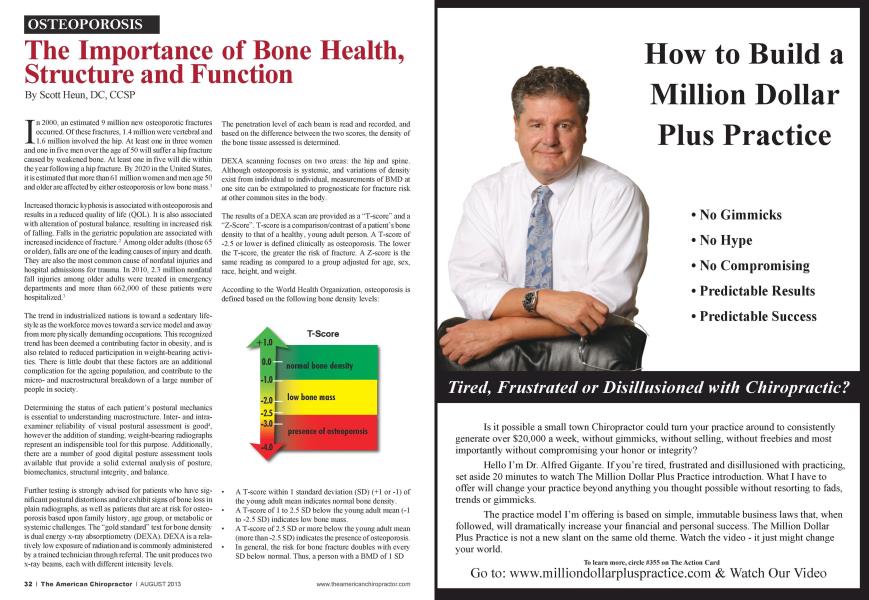
In 2000. an estimated 9 million new ostcoporotic fractures occurred. Of these fractures. 1.4 million were vertebral and 1.6 million involved the hip. At least one in three women and one in five men over the age of 50 will suffer a hip fracture caused by weakened bone. At least one in five will die within the year following a hip fracture. By 2020 in the United States, it is estimated that more than 61 million women and men age 50 and older arc affected by either osteoporosis or low bone mass.' Increased thoracic k\ phosis is associated with osteoporosis and results in a reduced quality of life (QOL). It is also associated with alteration of postural balance, resulting in increased risk of falling. Falls in the geriatric population arc associated with increased incidence of fracture.2 Among older adults (those 65 or older), falls arc one of the leading causes of injury and death. They arc also the most common cause of nonfatal injuries and hospital admissions for trauma. In 2010. 2.3 million nonfatal fall injuries among older adults were treated in emergency departments and more than 662.000 of these patients were hospitalized.3 The trend in industrialized nations is toward a sedentary lifestyle as the workforce moves toward a sen ice model and away from more physically demanding occupations. This recognized trend has been deemed a contributing factor in obesity, and is also related to reduced participation in weight-bearing activities. There is little doubt that these factors arc an additional complication for the ageing population, and contribute to the micro- and macrostnictural breakdown of a large number of people in society. Determining the status of each patient's postural mechanics is essential to understanding macrostnicturc. Inter- and intra-cxamincr reliability of visual postural assessment is good4, however the addition of standing, weight-bearing radiographs represent an indispensiblc tool for this purpose. Additionally, there are a number of good digital posture assessment tools available that provide a solid external analysis of posture, biomcchanics. structural integrity, and balance. Further testing is strongly advised for patients who have significant postural distortions and/or exhibit signs of bone loss in plain radiographs, as well as patients that are at risk for osteoporosis based upon family history, age group, or metabolic or systemic challenges. The "gold standard" test for bone density is dual energy x-ray absorptiomctry (DEXA). DEXA is a relatively low exposure of radiation and is commonly administered by a trained technician through referral. The unit produces two x-rav beams, each with different intensitv levels. The penetration level of each beam is read and recorded, and based on the difference between the two scores, the density of the bone tissue assessed is determined. DEXA scanning focuses on two areas: the hip and spine. Although osteoporosis is systemic, and variations of density exist from individual to individual, measurements of BMD at one site can be extrapolated to prognosticate for fracture risk at other common sites in the body. The results of a DEXA scan are provided as a "T-scorc" and a "Z-Scorc". T-scorc is a comparison/contrast of a patient's bone density to that of a healthy, young adult person. A T-scorc of -2.5 or lower is defined clinically as osteoporosis. The lower the T-scorc. the greater the risk of fracture. A Z-scorc is the same reading as compared to a group adjusted for age. sex. race, height, and weight. According to the World Health Organization, osteoporosis is defined based on the following bone density levels: A T-score within 1 standard deviation (SD) (+1 or -1) of the young adult mean indicates nonnal bone density. A T-scorc of 1 to 2.5 SD below the young adult mean (-1 to -2.5 SD) indicates low bone mass. A T-score of 2.5 SD or more below the young adult mean (more than -2.5 SD) indicates the presence of osteoporosis. In general, the risk for bone fracture doubles with every SD below nonnal. Thus, a person with a BMD of 1 SD below normal (T-scorc of-1) has twice the risk for bone fracture as a person with a normal BMD. A person with a T-scorc of -2 has four times the risk for bone fracture as a person with a normal BMD. When this information is known, people with a high risk for bone fracture can be treated with the goal of preventing future fractures. Severe osteoporosis is defined as having a bone density that is more tlian 2.5 SD below the young adult mean with one or more past fractures due to osteoporosis. The Z-score is your BMD as compared to an age-matched norm. Z-scorcs arc calculated in the same way. but the comparisons arc made to someone of the same age. sex. race, height, and weight.5 In weighting the value of the T-scorc and Z-scorc. the T-scorc is most important. The fact is that the aging population has an ever-greater incidence of ostcopenia and osteoporosis, and an ever-growing incidence of falls and the complications associated with these conditions. Therefore, in this authors opinion, the control group used to derive the Z-score presents a less valuable measure of macro- and microstructural health. According to the National Osteoporosis Foundation, women who arc taking an osteoporosis medication should have a DEXA scan every two years.'1 There is not. however, a firm consensus on this point, as in extreme cases, or very high-risk cases, more frequent testing is advised. Many insurance companies and HMOs resist testing patients until age 65. In light of the serious impact of this disease on patients, and the trend toward a more sedentary lifestyle in industrialized nations, testing should be done much earlier. A proactive approach could represent actual preventative healthcare. Furthermore, the initial radiographic screening done by most chiropractors is an important early detection tool to assess bone health and structural integrity. Due to many factors in the healthcare marketplace of 2013, chiropractors arc often the dc facto family physician for many individuals, and represent a direct portal of entry into the healthcare system. Chiropractors should be ever mindful of the nature of each patient's macro- and infrastructure in order to deliver safe, superior care and management of each patient's musculoskclctal system. In addition, chiropractors should fully evaluate the variety of clinical approaches to treating ostcopc-nia. osteoporosis, and abnormal posture in order to insure the delivery of the highest standard of patient care. There is broad consensus in the literature that weight-bearing activities produce healthier bone. The fact is that bone remodels to stress imposed (Wolfs law). The interrelationship of these two natural processes has a profound impact upon the human frame. Gravity can be friend or foe. depending upon the loading of the skeleton. Gross alignment or malalignmcnt of the skull, thorax, and pelvis have a profound impact upon the vertebral motor units, long bones, and the bones of the ankle and foot. Attention to postural alignment and. therefore, structural loading of the spine and articulated skeleton is essential to thorough patient care. Sustained abnormal posture produces microstructural changes to the vertebrae, and eventually, alterations in the architecture of the spine. For example, the end stage of forward head posture and concomitant hyperkyphosis is an ever-worscning breakdown of the thoracic spine, often resulting in extreme distortion of the torso and a perpetual progression of forward head and torso weight bearing. Absent a walker, patients arc unable to maintain upright posture. Further deterioration often leads to a fall, and the resulting grave consequences as described earlier, or life confined to a wheel chair. Enlisting gravitational force as a "friend" instead involves specific structured exercise, crgonomic considerations, and in instances of restricted spinal mobility, manipulative procedures to improve mobility and improve the overall weight-bearing posture. The safest and most effective form of spinal postural loading for purposes of improving bone density consistent with normal spinal structure is that undertaken with an "extension bias." 7 Extension exercises arc far superior to: A) flexion exercise. B) combined flexion and extension exercise, and C) no exercise at all." Isometric muscle contraction performed in the end range of skeletal extension, such as in pressing or pulling motions against an immovable stnicture while incorporating a concomitant firing of the spinal extensors in an optimized global spinal posture.'1 creates skeletal loading of the long bones by direct force production and. therefore, stimulation of bone growth. It also induces vertical vertebral loading via spinal extensor muscle contraction and reciprocal recniitment of all. secondary, and tertian muscles active in stabilizing the spine and torso stimulated by the effort. Exercise that is cither of low intensity or docs not involve skeletal loading, primarily or secondarily as described earlier, is largely ineffective in countering bone loss or improving bone density in postmcnopausal individuals.10 In this authors opinion, based upon experience, low-intensity muscular load- ing is also ineffective in altering global postural weight bearing and in improving core strength. In order to improve posture and optimize sagittal balance, optimized maximal loading of the motor units and related musculotendinous tissues must be consistently employed. Eccentric exercise lias many benefits over either concentric or isometric exercise. The primary benefit is the fact tliat the metabolic demand of eccentric exercise is less than other forms of training. Also, in light of the fact that muscles are from 1 to 1.5 times stronger in eccentric contraction than concentric contraction, the potential for safe maximum loading in the performance of eccentric loading is tremendous. In approaching the patient with abnormal posture and. therefore, altered weight bearing, further complicated by muscular de-conditioning, the pin sician must design long bone and skeletal stimulation loading sufficient to induce desired bone density increases, while safely loading the musculoskeletal system to minimize negative consequences. One of the most advanced methods for safely loading the musculoskeletal system involves whole body vibration (WBV). There are a number of vendors that supply these products, PowcrPlatc R and WAVE R Exercise arc two I am familiar with tliat provide a wealth of infonnation on their websites about WBV training. In some instances, highly supervised weight training using conventional equipment can be employed. However, the risk is high for injury and the learning curve for performing most exercises or maneuvers is demanding. Static/isometric loading in optimized biomcchanical positions and incorporating coaching to insure maximum possible recruitment is advisable. Specific equipment to achieve desirable loading with a less demanding learning curve and reduced risk of injury is available from Performance Health Systems. Inc.. which produces a commercial product known as bioDcnsity R. The decision to address microstnictural challenges as well as gross postural distortions or niacrostnictural dysfunction is one each practicing clinician must address. This author has witnessed the tremendous benefits of integrating this comprehensive approach in clinical practice and what it means to patient's lives. ► To view references go to page 56 Dr. ScottHeun isapractidngcliimpractor inNapa, CA with over 30wars of clinicalexperience. He is also the co-founder of B'Strong4I.ife^ mrw.bstmng4life.com a rwolulioncay company dedicated to imprm'ing core strength, balance and bone heallh using a proprietary system of analysis, training and patient management. In addition, he is also a sought afler chiropractic advisor and mentor, specializing in patient-centered practice and doctor patient communication mrw.cliirvpracticenientoring.com Dr. Heun can he reached at drscotldhstrong4life.com ► (\mtimwcl from page 37 1. International Osteoporosis Foundation 2011 2. Influence of Sagittal Balance and Physical Ability Associated with Exercise On Quality of Life in Middle Aged and Elderly People Arch Ostcoporos. 2011 vol. 6(1-2) pp 13-20 3. Hornbrook MC. Stevens VJ. Wingficld DJ. Hollis JF. Green-lick MR. On MG. Preventing falls among community-dwelling older persons: results from a randomized trial. The Gcronlologisl 1994:34(l):16-23. 4. "Inler-examinar Rcliabilly of the Right-Handed Cartesian Orthogonal Coordinate System for Use of Listing Postural Distortions" Bradbury and McVeigh Logan College of Chiropractic- Senior Research 1999-Dec-10 5. World Health Organization 2012 6. National Osteoporosis Foundation 2012 7. BStrong4Life R Protocol 2009-2013 Scott J. Hcuii. DC. CCSP. Pern Cammisa. DC 8. Archives of Physical Medicine and Rehabilitation. 1984 Oct:65(10):593-6. 9. J Manipulative Physiol Ther. 1996 Jul-Aug: 19(6):398-405. A normal sagittal spinal configuration: a desirable clinical outcome. Harrison DD. Troyanovich SJ. Harrison DE. Janik TJ. Murphy DJ. Eur Spine J. 2002 Jumll(3):287-93. Epub 2001 Nov 1. How do anterior/posterior translations of the thoracic cage affect the sagittal lumbar spine, pelvic till, and thoracic kyphosis? Harrison DE. Caillict R. Harrison DD. Janik TJ. Eur Spine J. 2011 September: 20(Suppl 5): 699-703. Published online 2011 August 3. doi: 10.1007/s00586-011-1938-8 PMCID:PMC3175932 Sagittal imbalance cascade for simple degenerative spine and consequences: algorithm of decision for appropriate treatment J. C. Lc Huec.corrcsponding author 1 S. Charosky.2.4 C. Barrcy.3 J. Rigal. 1 and S. Aunoblel 10. Mayo Clin Proc. 1989 Jul: 64(7): 762-9.Efficacy of non-loading exercises in prevention of vertebral bone loss in postmcnopausal women: a controlled trial. Sinaki M. Wanner HW. Offord KP. Hodgson SF.