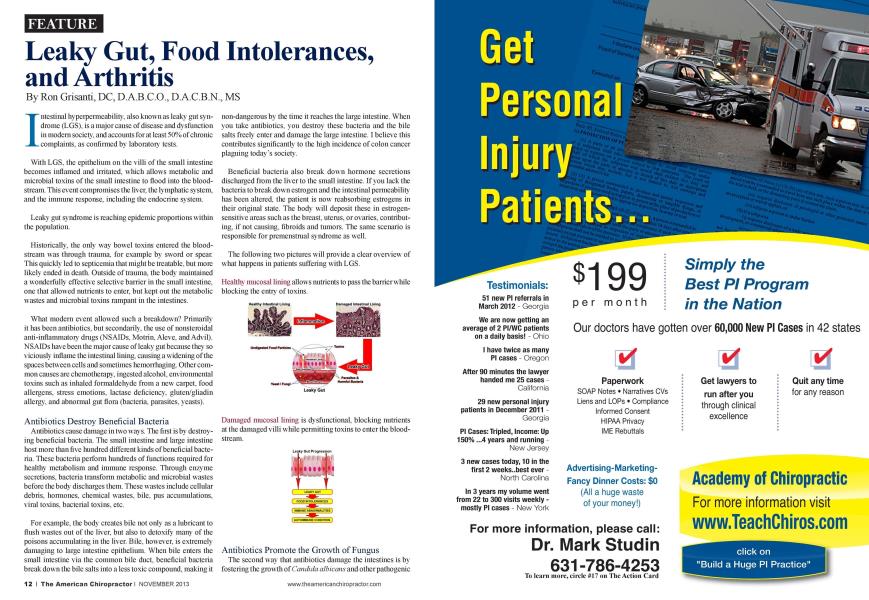
I ntcstinal hypcrpcnncability. also known as leak}' gut syndrome (LGS). is a major cause of disease and dysfunction in modem society, and accounts for at least 50% of chronic complaints, as confirmed by laboratory tests. With LGS. the epithelium on the villi of the small intestine becomes inflamed and irritated, which allows metabolic and microbial toxins of the small intestine to flood into the bloodstream. This event compromises the liver, the lymphatic system, and the immune response, including the endocrine system. Leaky gut syndrome is reaching epidemic proportions within the population. Historically, the only way bowel toxins entered the bloodstream was through trauma, for example by sword or spear. This quickly led to scpticcmia that might be treatable, but more likely ended in death. Outside of trauma, the body maintained a wonderfully effective selective barrier in the small intestine, one that allowed nutrients to enter, but kept out the metabolic wastes and microbial toxins rampant in the intestines. What modem event allowed such a breakdown? Primarily it has been antibiotics, but secondarily, the use of nonstcroidal anti-inflammatory dnigs (NSAIDs. Motrin. Alevc. and Advil). NSAIDs have been the major cause of leaky gut because they so viciously inflame the intestinal lining, causing a widening of the spaces between cells and sometimes hemorrhaging. Other common causes are chemotherapy, ingested alcohol, environmental toxins such as inhaled formaldehyde from a new carpet, food allergens, stress emotions, lactasc deficiency, glutcn/gliadin allergy, and abnormal gut flora (bacteria, parasites, yeasts). Antibiotics Destroy Beneficial Bacteria Antibiotics cause damage in two ways. The first is by destroying beneficial bacteria. The small intestine and large intestine host more than five hundred different kinds of beneficial bacteria. These bacteria perfonn hundreds of functions required for health} metabolism and immune response. Through enzyme secretions, bacteria transform metabolic and microbial wastes before the body discharges them. These wastes include cellular debris, hormones, chemical wastes, bile, pus accumulations, viral toxins, bacterial toxins, etc. For example, the body creates bile not only as a lubricant to flush wastes out of the liver, but also to detoxify many of the poisons accumulating in the liver. Bile, however, is extremely damaging to large intestine epithelium. When bile enters the small intestine via the common bile duct, beneficial bacteria break down the bile salts into a less toxic compound, making it non-dangerous by the time it reaches the large intestine. When you take antibiotics, you destroy these bacteria and the bile salts freely enter and damage the large intestine. I believe this contributes significantly to the high incidence of colon cancer plaguing today's society. Beneficial bacteria also break down hormone secretions discharged from the liver to the small intestine. If you lack the bacteria to break down estrogen and the intestinal permeability has been altered, the patient is now rcabsorbing estrogens in their original state. The body will deposit these in estrogen-sensitive areas such as the breast, uterus, or ovaries, contributing, if not causing, fibroids and tumors. The same scenario is responsible for premenstrual syndrome as well. The following two pictures w ill provide a clear overview of what happens in patients suffering with LGS. Healthy mucosal lining allows nutrients to pass the barrier while blocking the entry of toxins. Damaged mucosal lining is dysfunctional, blocking nutrients at the damaged villi while permitting toxins to enter the bloodstream. Antibiotics Promote the Growth of Fungus The second way that antibiotics damage the intestines is by fostering the growth of Candida albicaiis and other pathogenic fungi and yeast. This event, more than any other, precipitates LGS. In a healthy situation, the small intestine epithelium maintains tight cell junctions, which contributes to the physical barrier involved in intestinal absorption. In addition to the pin sical barrier, there is an important chemical barrier within the mucus that contains immune agents, which neutralize any toxin that comes in contact. Candida exudes an aldehyde secretion, which causes small intestine epithelial cells to shrink. This allows intestinal toxins to infiltrate through the epithelium and into the blood. The secondary barrier—immune agents in the epithelial mucus—remain the sole agent for neutralization. Eventually, the immune system becomes exhausted rising to this challenge. The damage done by Candida is to the intestinal epithelial barrier, allowing the absorption of serious toxic agents and chemicals, which then enter the blood and affect numerous organs, including the brain. Food Intolerance: The Complicating Factor When the integrity of the intestinal barrier has been compromised, intestinal toxins are not the only pathogens to be absorbed. The barrier, in a healthy state, selectively allows digested nutrients to enter the small intestine when all is ready. The most common food reactions are dairy, eggs, gluten grains (wheat, oats. rye), com. beans (especialh soy), and nuts. There arc seldom real allergies to meat. rice, millet, vegetables, or fruit, although an allergy to garlic is not uncommon. The Role of the Liver and Lymphatic System The metabolic and microbial toxins that enter the bloodstream during leakv gut end up in the liver, which lias the job of detoxifying and discharging the poisons. With lcak> gut. nutrients can be absorbed before they arc fully digested. The body"s immune response, through specific antigen-antibody markers, will tag some of these foods as foreign irritants. Every time that particular food touches the cpithclia an inflammatory immune response is mounted, which further damages the epithelial lining. What started as a Candida irritation with shrinking of the cells now has been complicated with active inflammation every time a particular food is eaten. Food intolerances arc a common secondary problem to C 'andida. and if present, will maintain the leak}- gut continuously, even if the Candida is eradicated. The following is an IgG4 food antibody test. IgG4 antibodies arc associated with delayed hypcrsensitivity reactions, which are the most common—yet most difficult to detect—type of food reaction. These delayed or "hidden" food reactions can cause a variety of chronic symptoms. Since IgG4 reactions occur several hours or even days later, there may be no obvious association between consuming a food and an adverse reaction. Food IgG4 levels increase in response to the presence of the food antigens that penetrate a weakened intestinal barrier and enter the bloodstream. IgG4 antibodies combine with specific food antigens to form food immune complexes, which cause the problems associated with delayed allergic responses. The complexes can cause inflammatory reactions at various sites in the body, including the small and large intestines, skin, kidneys, ears, sinuses, head, lungs, and joints. Under normal conditions, the liver is taxed just by processing the daily metabolic wastes created by cell and organ activity. Imagine the further load created by dumping serious intestinal toxins on a regular basis. There is a point when the liver becomes saturated: it cannot further detoxify the poisons, and they are returned to the blood circulation. The blood has sophisticated mechanisms for preserving chemical homeostasis, and will diffuse as much of the toxic chemicals and physical debris into the interstitial fluids as is possible. From here, the Ordering Physician: Ronald Grisanti. DC Date Received: 3/5/2013 Date Reported: 3/11/2013 0075 IgG4 Food Antibodies (90 Antigens) Dairy/ Meat / Results Response Class Legumes Results Response Poultry ng/mL ng/mL Beef <10 Bean. String <10 Casein 207 Mod +3 Lentil <10 Chicken 10 Lima Bean <10 Egg. White 466 Mod +3 Navy Bean 8 Egg. Yolk 466 Mod +3 Pea. Green <10 Lamb 23 Peanut 16 Milk 286 Mod +3 Pinto Bean <10 Pork <10 Soybean <10 Turkey 44 Mild + 1 Fish/Shellfish Miscellaneous Aspcrgillus <10 lymphatic system will attempt to collect and neutralize the toxins, but when the body is unable to send the toxins to the liver, it essentially becomes toxic. Microbes grow and develop: hence, there can be chronic lymphatic swelling, especially in children. Cher time, toxins will be forced into distal connective tissue around muscles and joints, causing fibromyalgia. or into the cells, which can precipitate genetic mutation and ultimately cancer. Stress to the Immune and Endocrine Systems The immune system is stressed in three major ways. First, it occurs at the site of the intestinal mucosa. As toxins and food antigens brush up against the mucosa. the immune system mobilizes to neutralize the toxins. Much of this work normally would have been done by beneficial bacteria, which have been destroyed by antibiotics. For toxins that make it to the mucosa. the body will tag them with a chemical secretory immunoglobu-lin A (SIgA). which attracts macrophages and otherwhite blood cells to consume the toxins. It is not long before this immune response is overwhelmed and depicted. This can be measured directly with a stool or saliva test for the intestinal SIgA level. The second strcssor happens in the liver and lymphatic system, which, also overwhelmed, puts demands on the immune system. The third strcssor is a consequence: as the immune response diminishes, more microbes (viruses, bacteria, and fungi) multiply, allowing for a chronic state of infection. The most important organ in the production of immune agents seems to be the adrenal gland, and leaky gut syndrome slowly diminishes adrenal function. In the earlv and middle stages, there is actually an adrenal excess, as measured by excess cortisol output. Eventually, cortisol levels drop, and one now has exhaustion. The Role of the Digestive Tract Candida nourishes when the terrain in the intestines favors it. Just killing Candida is usually not successful because the chemistry and vitality of the terrain has not been normalized, and Candida returns. Antibiotics are the original cause of the change on the terrain. By killing acid-forming bacteria (for example. Lactobacillus bacteria produce lactic acid), the environment becomes alkaline, which promotes C "anclida. An- tibiotics and chronic illness reduce stomach acid production, contributing to the alkalinity and allowing for poor digestive absorption. In fact, many people with LGS arc malnourished and will lose excessive weight no matter how health) the food is that they eat. The idea that Lactobacillus supplementation is all that is required after taking antibiotics is somewhat delusional: in fact, most of the Lactobacillus from supplementation does not survive in the intestine due to poor terrain. Just to make sure you have a full understanding of the seriousness of LGS. the following is a summary: When the gut is inflamed, it docs not secrete digestive enzymes to digest foods properly or absorb nutrients and foods properly. The result can be indigestion with gas and bloating called irritable bowel syndrome (IBS). When large food particles are absorbed, food allergies and new symptoms arc created (e.g.. IBS. gallbladder disease, arthritis, or fibromyalgia). When the gut is inflamed, carrier proteins are damaged, so malabsorption and nutrient deficiencies occur. These deficiencies slow down the ability of the gut to heal and can cause any number of other symptoms (e.g.. magnesium deficiency—induced angina or gut spasms: chromium deficiency—induced high cholesterol or sugar cravings: zinc deficiency—induced prostatitis or lack acid formation). When the detoxification pathways that line the gut arc compromised, chemical sensitivity can arise. Further more, the leakage of toxins overburdens the liver so that the bod) is less able to handle everyday chemicals in foods, water, and air. Now many foods can cause symp toms that never did before because the gut"s detoxifica tion (liver) system is unable to cope with the hundreds of chemical additives, dyes, colorings, preservatives, and pesticides common in our foods. When the gut lining is inflamed, the protective coating of the gut antibodies can be lost. With loss of the secre tory immunoglobulin A(SIgA). the body becomes more vulnerable to infections in the intestines from bacteria, viruses, parasites, and yeast and they become resistant to treatment. Ironically, the more resistant the bugs become, the more high-powered antibiotics doctors prescribe, resulting in more overgrowth of resistant fungi (Candida). As the unwanted bugs grow, the gut becomes more inflamed and "leaky" initiating a vicious cycle of worsening condition, and the major cause of so mam "incurable" diseases. When the intestinal lining is inflamed, bacteria and yeast can translocate. In other words, they can pass from the gut cavity into the bloodstream and set up infection any where else in the body, including the brain. This is often the mysterious and undiagnosed cause of infections in the teeth and gums, bones, prostate, bladder, and sinuses. With the formation of antibodies, the food antigens that leak across the gut wall can sometimes resemble the natural antigens on tissues. Protective antibodies will then attack the antigens, as they should, and the tissues, causing further damage. This, in fact, may be a primary reason for why autoimmune diseases begin. Lupus, multiple sclerosis, rheumatoid arthritis, myocarditis, iritis, and thyroiditis arc some of the members of this ever-growing category of mysteriously "incurable" autoimmune diseases. References: Farliadi A. Banan A. Fields J. Keshavarzian A. Intestinal barrier: an interface between health and disease. J Gastrocntcrol Hcpatol. 2003 May: 18(5):479-97. ■ Viljocn M. Panzer A. Willcmsc N. Gastrointestinal hypcrpcrmc- ability: a review. East Afr Mcd J. 2003 Jun;8O(6):324-3O. > Darlington LG. Ramsey NW. Review of dietary therapy for rheu matoid arthritis. Br J Rhcumatol. 1993 Jun:32(6):5O7-14. van dc Laar MA. van dcr Korst JK. Food intolerance in rheumatoid arthritis. I. A double blind, controlled trial of the clinical effects of elimination of milk allergens and a/.o dyes. Ann Rheum Dis. 1992 Mar.51(3):298-3O2. > van dc Laar MA. Aalbcrs M. Brains FG. van Dinthcr-Jansscn. Food intolerance in rheumatoid arthritis. II. Clinical and histological aspects. Ann Rheum Dis. 1992 Mar:51(3):3O3-<i. Kjcldscn-Kragh J. Forrc O. |Diet and rheumatoid arthritis] Tidsskr Nor Laegcforcn. 1989 Jan 10:109(l):29-32. ■ Pricr A. |Effccts of dietetic manipulations on the course of rheuma toid arthritis | Pressc Mcd. 1988 Jun ll:17(23):1181-3. Panush RS. Possible role of food sensitivity in arthritis. Ann Allergy. 1988 Dcc:61(6 Pt 2):31-5. ■ Zussman BM. Food hypersensitivity simulating rheumatoid arthritis. South Mcd J. 1966Aug:59(8 CrycrB. Kimmcy MB. Gastrointestinal side effects of nonstcroidal anti-inflammatory drags. Am J Mcd. 1998:1O5(1B):2OS-3OS. Price AH. Fletcher M. Mechanisms of NSAID-induccd gastrocn-tcropathy. Drags. 1990:40 Suppl 5:1-11. Zalcv AH. Gardiner GW. Warren RE. NSAID injury to the small intestine. Abdom Imaging. 1998:23(l):40-4. Hirschowitz BI. Nonstcroidal anti-inflammatory drags and the gastrointestinal tract. Gastrocnterologist. 1994:2(3):207-23. 1 Wallace JL. The 1994 Merck Frosst Award. Mechanisms of nonstcroidal anti-inflammatory drag (NSAID) induced gastrointestinal damage potential for development of gastrointestinal tract safe NSAIDs. Can J Physiol Pharmacol. 1994:72(12):1493-8. ■ Aabakkcn L. Review article: non-stcroidal. anti-inflammatory drags—the extending scope of gastrointestinal side effects. Aliment Pharmacol Thcr. 1992:6(2): 143-62. Fuller R. Hirosc-Pastor E. Levy M. Zatcrka S. Massuda HB. Eisig JN. YoshinariNH. Gastrointestinal damage in ostcoarthritis patients. Rev Hosp Clin Fac Mcd Sao Paulo. 1997:52(2):47-50. Larkai EN. Smith JL. Lidsky MD. Graham DY. Gastroduodcnal nutcosa and dyspeptic symptoms in arthritic patients during chronic nonstcroidal and anti-inflammatory drag use. Am J Gastrocnterol. 1987;82(ll):1153-8. Davies NM. Review article: non-stcroidal anti-inflammatory drug- induccd gastrointestinal permeability. Aliment Pharmacol Thcr. 1998;12(4):303-20. Ronald Grisanti D.C., D.A.B.C.O., D.A.C.B.N., M.S., is medical director of Functional Medicine University. If interested in improving vour diagnostic skills and increasing your community reputation and recognition, we strongly recommend subscribing to our Free Clinical Rounds Series. Tliese challenging case studies will give you the unique opportunity to test your clinical skills and, at the same time, improve your ability to handle many of the most difficult cases. Go to the following link to get your free access: www.ClinicalRounds.com.