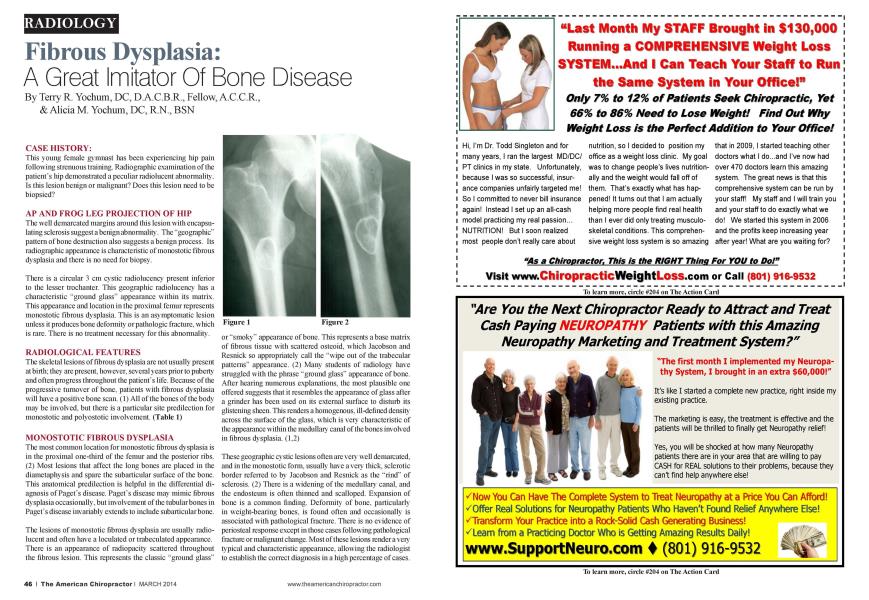
CASE HISTORY: This young female gymnast has been experiencing hip pain following strenuous training. Radiographic examination of the patient's hip demonstrated a peculiar radioluccnt abnormality. Is this lesion benign or malignant? Does this lesion need to be biopsicd? AP AND FROG LEG PROJECTION OF HIP The well demarcated margins around this lesion with encapsulating sclerosis suggest a benign abnormality. The "geographic" pattern of bone destruction also suggests a benign process. Its radiographic appearance is characteristic of monostotic fibrous dysplasia and there is no need for biopsy. There is a circular 3 cm cystic radiolucency present inferior to the lesser trochantcr. This geographic radioluccncy has a characteristic "ground glass" appearance within its matrix. This appearance and location in the proximal femur represents monostotic fibrous dysplasia. This is an asymptomatic lesion unless it produces bone deformity or pathologic fracture, which is rare. There is no treatment necessary for this abnormality. RADIOLOGICAL FEATURES The skeletal lesions of fibrous dysplasia arc not usually present at birth: they arc present, however, several years prior to puberty and often progress throughout the patient's life. Because of the progressive turnover of bone, patients with fibrous dysplasia will have a positive bone scan. (1) All of the bones of the body may be involved, but there is a particular site predilection for monostotic and polyostotic involvement. (Table 1) MONOSTOTIC FIBROUS DYSPLASIA The most common location for monostotic fibrous dysplasia is in the proximal one-third of the femur and the posterior ribs. (2) Most lesions that affect the long bones arc placed in the diamctapln sis and spare the subarticular surface of the bone. This anatomical predilection is helpful in the differential diagnosis of Pagct"s disease. Pagcts disease may mimic fibrous dysplasia occasionally, but involvement of the tubular bones in Pagcfs disease invariably extends to include subarticular bone. The lesions of monostotic fibrous dysplasia are usually radio-lucent and often have a loculatcd or trabcculatcd appearance. There is an appearance of radiopacity scattered throughout the fibrous lesion. This represents the classic "ground glass" or "smoky" appearance of bone. This represents a base matrix of fibrous tissue with scattered ostcoid. which Jacobson and Rcsnick so appropriately call the "wipe out of the trabecular patterns" appearance. (2) Many students of radiology have struggled with the phrase "ground glass" appearance of bone. After hearing numerous explanations, the most plausible one offered suggests that it resembles the appearance of glass after a grinder has been used on its external surface to disturb its glistening sheen. This renders a homogenous, ill-defined density across the surface of the glass, which is very characteristic of the appearance within the medullary canal of the bones involved in fibrous dysplasia. (1.2) These geographic cystic lesions often arc very well demarcated, and in the monostotic form, usually have a very thick, sclerotic border referred to by Jacobson and Rcsnick as the "rind" of sclerosis. (2) There is a widening of the medullary canal, and the endostcum is often thinned and scalloped. Expansion of bone is a common finding. Deformity of bone, particularly in weight-bearing bones, is found often and occasionally is associated with pathological fracture. There is no evidence of pcriostcal response except in those cases following pathological fracture or malignant change. Most of these lesions render a very typical and characteristic appearance, allow ing the radiologist to establish the correct diagnosis in a high percentage of cases. Table I Radiological Features of Fibrous Dvsplasia MONOSTOTIC Proximal femur, posterior ribs Diametaphyseal Geographic Lucent, smoky ("ground glass") Thick sclerotic margin ("rind") Occasionally scptatcd ("soapbubble") Expansion Cortical thinning and scalloping Elongated lesion Pathological fracture POLYOSTOTIC Multiple lesions: may be unilateral Pscudofractures Deformities Femur: coxa vara. shepherd "s crook Rib: cxtraplaural sign Pelvis: protnisio acctabulae Spine rarely involved COMPLICATIONS Malignancy (0.5%) Fractures Deformities References Yochum TR. Rowe LJ: The Essentials of Skeletal Radiology, 3rd ed.. Baltimore. Williams & Wilkins. 2005. Rcsnick D.: Diagnosis of Bone and Joint Disorders, cd. 4. Phila delphia. WB Saunders. 2002. Dr. Terry R. Yochum is a second generation chiropractor and a Cum Laude Graduate ofXational College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rocky Mountain Chiropraclic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology at the University ofColorado School of.\ ledicine, Denver, CO. Dr. Yochum can be reached at 1-303-940-9400 or by e-mail at dcradO99(daol.com Dr. Alicia M. Yochum is a third generation chiropractor and 2011 Suma Cum Laude Graduate of Logan College of Chiropractic, as well as a Registered Xurse. She is in a Radiology residency at Logan College in St. Louis, MO. She can be reached at alicia.yochum'Q gmail.com.