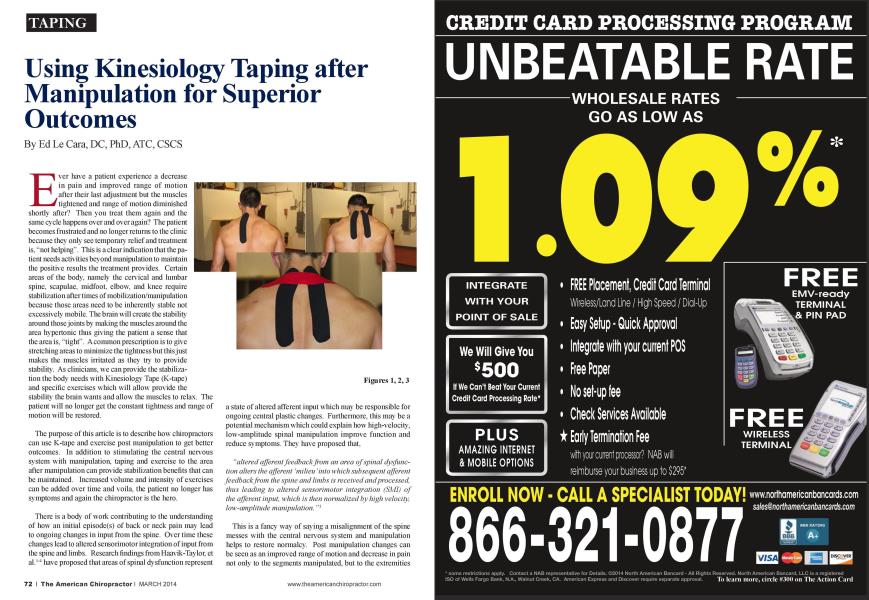
E ver have a patient experience a decrease in pain and improved range of motion after their last adjustment but the muscles tightened and range of motion diminished shortly after? Then you treat them again and the same cycle happens over and over again? The patient becomes fnistratcd and no longer returns to the clinic because they only sec teniporan relief and treatment is. "not helping". This is a clear indication that the patient needs activities beyond manipulation to maintain the positive results the treatment provides. Certain areas of the body, namely the cervical and lumbar spine, scapulae, midfoot. elbow, and knee require stabilization after times of mobilization/manipulation because those areas need to be inherently stable not excessively mobile. The brain will create the stability around those joints by making the muscles around the area hypcrtonic thus giving the patient a sense that the area is. "tight". A common prescription is to give stretching areas to minimize the tightness but this just makes the muscles irritated as they try to provide stability. As clinicians, we can provide the stabilization the body needs with Kinesiologv Tape (K-tapc) and specific exercises which will allow provide the stability the brain wants and allow the muscles to relax. The patient will no longer get the constant tightness and range of motion will be restored. The purpose of this article is to describe how chiropractors can use K-tapc and exercise post manipulation to get better outcomes. In addition to stimulating the central nervous system with manipulation, taping and exercise to the area after manipulation can provide stabilization benefits that can be maintained. Increased volume and intensity of exercises can be added over time and voila. the patient no longer has symptoms and again the chiropractor is the hero. There is a body of work contributing to the understanding of how an initial cpisodc(s) of back or neck pain may lead to ongoing changes in input from the spine. Over time these changes lead to altered sensorimotor integration of input from the spine and limbs. Research findings from Haavik-Taylor. ct al.M have proposed that areas of spinal dysfunction represent a state of altered afferent input which may be responsible for ongoing central plastic changes. Furthermore, this may be a potential mechanism which could explain how high-velocity, low-amplitude spinal manipulation improve function and reduce symptoms. They have proposed that. "altered afferent feedback from an area of spinal dysfunction alters the afferent 'milieu 'into which subsequent afferent feedback from the spine and limbs is received and processed, thus leading to altered sensorimotor integration (SMI) of the afferent input, which is then normalized by high velocity, low-amplitude manipulation. "' This is a fancy way of saying a misalignment of the spine messes with the central nervous system and manipulation helps to restore normalcy. Post manipulation changes can be seen as an improved range of motion and decrease in pain not only to the segments manipulated, but to the extremities as well. Unfortunately, even after the pain is gone and the tissue lias healed, the muscles already learned what it is like to be hurt. Therefore the benefit is only temporary. Previously injured muscles need proper stimulus to be reset so they can contract properly. K-taping can be one piece of the puzzle that contributes to teaching the muscles to be nonnal again. Callaglian ct al5 demonstrated that K-taping may be an. "efficacious therapy due to subtle mechanisms affecting the brain, not just because it gives mechanical support...". The tape provides afferent mcchanorcccptor stimulus to the brain and the brain will perceive stability. In the example of the cervical spine, if the area is stable, the brain docs not have to tighten up the muscles around the neck to provide stability. In addition, the patient will be reminded to keep their head in a good posture position that leads to other benefits. Anytime I manipulate or use myofascial release to areas that inherently need stability I follow manipu- lation with something to stimulate the central nervous system. In the cervical spine. I use a simple "h" taping technique (Figure 1-3). With this new sense of stability from the tape, it is easy to the have the patient perform exercises maintain the stability through muscular contraction. For the cervical spine. I like activating the deep cervical flexors for 7 second holds (Figure 4). Start with 5 repetitions and work up to 2 sets of 10 repetitions. Remind the patient to breathe through the diaphragm while they arc performing these exercises, in through the nose for 4 seconds and out through their nose for 6 seconds. If they cant breathe properly, the exercise is too difficult. How long does the muscular normalcy stay? I have found that those who are more active tend to sec greater benefits from the care I provide. Have patients increase their cardiovascular activity as well if they arc not active. I propose that anytime one manipulates or mobilizes an area tliat is required to be stable, use K-tapc post manipulation to increase the afferent stimulation to the brain. The brain in turn will allow for pain mitigation and improved motor control thus eliminating the need for the muscles to provide stability to the area (be hyperactive). If motor control exercises are used in conjunction with manipulation and taping, an even better effect can be experienced. References: 1. Haavik-Taylor H. Murphy B. Altered central integration of dual somatosensory input after cervical spine manipulation. J Manipulative Physiol Thcr 2010a;33(3): 178-88. Haavik-Taylor H. Murphy B. The effects of spinal manipula tion on central integration of dual somatosensory input observed after motor training: a crossover study. J Manipulative Physiol Thcr 201()b:33(4):261-72. Haavik H. Murphy B. Subclinical neck pain and Ihe effect of cervical manipulation on elbow joint position sense. J Manipulative Physiol Thcr 2011:34:88-97. 4. Haavik-Taylor H. Murphy B. The effects of spinal manipulation on central integration of dual somatosensory input observed follow ing motor training: a crossover study. J Manipulative Physiol Ther 201()c:33:261-72. 5. Callaghan. MJ ct al. Effects of patcllar taping on brain activity dur ing knee joint proprioccption tests using functional magnetic resonance imaging. Physical Therapy 2012:92(6):821-830. Ed Le Cara, DC, PhD, ATC, CSCS is board certified in sports medicine and rehabilitation. He is a chiropractic clinician, educator anil on the medical advisory board for Rocktape. lie provides live and online education for move- menl professionals al'www. IleallhamlU'ellnessPmvklers.com. To contact him, email at drlecaraaSportsI'lusBayArea.com or follow on Twitter: (djjdrlecara. He hosts a monthly wehinar demonstrating different taping applications and answers questions. Ix>ok on Google Hangouts under 'Basics of Kinesiology Taping'for his next event.