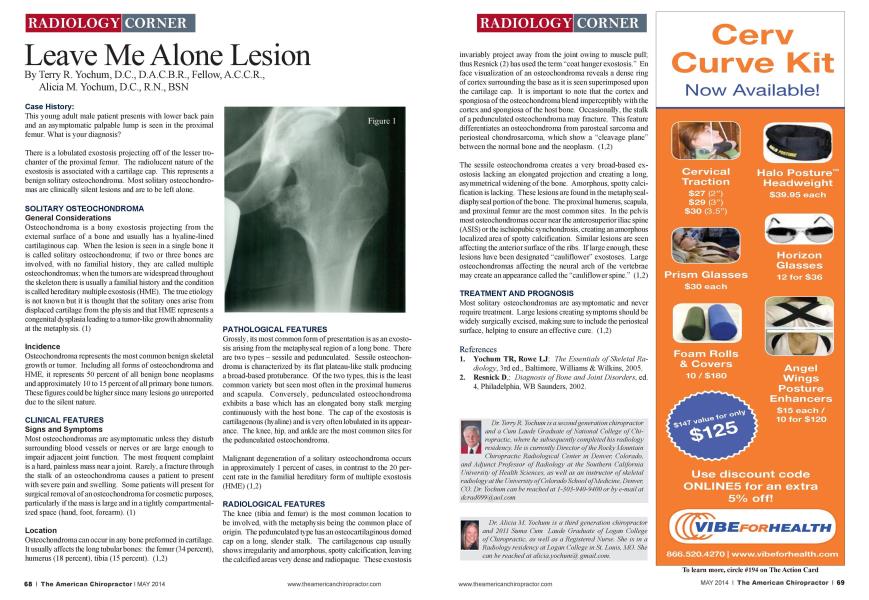
Case History: This young adult male patient presents with lower back pain and an asymptomatic palpable lump is seen in the proximal femur. What is your diagnosis? There is a tabulated exostosis projecting off of the lesser trochanter of the proximal femur. The radiolucent nature of the exostosis is associated with a cartilage cap. This represents a benign solitary ostcochondroma. Most solitary osteochondromas are clinically silent lesions and are to be left alone. SOLITARY OSTEOCHONDROMA General Considerations Ostcochondroma is a bom exostosis projecting from the external surface of a bone and usually has a hyaline-lined cartilaginous cap. When the lesion is seen in a single bone it is called solitary ostcochondroma: if two or three bones arc involved, with no familial history, they arc called multiple ostcochondromas: when the tumors arc widespread throughout the skeleton there is usually a familial history and the condition is called hereditary multiple exostosis (HME). The tme etiology is not known but it is thought that the solitary ones arise from displaced cartilage from the physis and that HME represents a congenital dysplasia leading to a tumor-like growth abnormality at the mctaphysis. (1) Incidence Ostcochondroma represents the most common benign skeletal growth or tumor. Including all forms of ostcochondroma and HME. it represents 50 percent of all benign bone neoplasms and approximately 10 to 15 percent of all primary bone tumors. These figures could be higher since many lesions go unreportcd due to the silent nature. CLINICAL FEATURES Signs and Symptoms Most ostcochondromas are asymptomatic unless they disturb surrounding blood vessels or nerves or arc large enough to impair adjacent joint function. The most frequent complaint is a hard, painless mass near a joint. Rarely, a fracture through the stalk of an ostcochondroma causes a patient to present with severe pain and swelling. Some patients will present for surgical removal of an ostcochondroma for cosmetic purposes, particularly if the mass is large and in a tightly compartmentalized space (hand. foot, forearm). (1) Location Ostcochondroma can occur in any bone preformed in cartilage. It usually affects the long tubular bones: the femur (34 percent), humenis (18 percent), tibia (15 percent). (1,2) PATHOLOGICAL FEATURES Grossly, its most common form of presentation is as an cxosto-sis arising from the mctaphyseal region of a long bone. There arc two types - sessile and pcdunculatcd. Sessile ostcochon-droma is characterized by its flat plateau-like stalk producing a broad-based protuberance. Of the two types, this is the least common variety but seen most often in the proximal humerus and scapula. Conversely, pcdunculatcd ostcochondroma exhibits a base which has an elongated bony stalk merging continuously with the host bone. The cap of the exostosis is cartilagcnous (hyaline) and is very often lobulatcd in its appearance. The knee. hip. and ankle arc the most common sites for the pcdunculated ostcochondroma. Malignant degeneration of a solitary ostcochondroma occurs in approximately 1 percent of cases, in contrast to the 20 percent rate in the familial hereditary form of multiple exostosis (HME)(1.2) RADIOLOGICAL FEATURES The knee (tibia and femur) is the most common location to be involved, with the mctaphysis being the common place of origin. The pcdunculatcd type has an ostcocartilaginous domed cap on a long, slender stalk. The cartilagcnous cap usually shows irregularity and amorphous, spotty calcification, leaving the calcified areas very dense and radiopaquc. These exostosis invariably project away from the joint owing to muscle pull; thus Rcsnick (2) has used the term "coat hanger cxostosis." En face visualization of an ostcochondroma reveals a dense ring of cortex surrounding the base as it is seen superimposed upon the cartilage cap. It is important to note that the cortex and spongiosa of the ostcochondroma blend imperceptibly with the cortex and spongiosa of the host bone. Occasionally, the stalk of a pcdunculatcd ostcochondroma may fracture. This feature differentiates an ostcochondroma from parostcal sarcoma and pcriosteal chondrosarcoma. which show a "cleavage plane" between the normal bone and the neoplasm. (1.2) The sessile ostcochondroma creates a very broad-based ex-ostosis lacking an elongated projection and creating a long, asymmetrical widening of the bone. Amorphous, spotty calcification is lacking. These lesions arc found in the mctapln seal-diaphyseal portion of the bone. The proximal humcrus. scapula, and proximal femur arc the most common sites. In the pelvis most osteochondromas occur near the anterosupcrior iliac spine (ASIS) or the ischiopubic synchondrosis. creating an amorphous localized area of spotty calcification. Similar lesions arc seen affecting the anterior surface of the ribs. If large enough, these lesions have been designated "cauliflower" exostoscs. Large osteochondromas affecting the neural arch of the vertebrae may create an appearance called the "cauliflower spine." (1.2) TREATMENT AND PROGNOSIS Most solitary' osteochondromas are asymptomatic and never require treatment. Large lesions creating symptoms should be widely surgically excised, making sure to include the pcriosteal surface, helping to ensure an effective cure. (1.2) References Yochum TR, Rowe LJ: The Essentials of Skeletal Ra diology. 3rd cd.. Baltimore. Williams & Wilkins. 2005. Rcsnick D.: Diagnosis of Bone and Joint Disorders, ed. 4. Philadelphia. WB Saundcrs. 2002. Dr. Terry R. Yochum is a second generation chiropractor and a Cum Laude Graduate ofXational College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology at the University of Colorado School of Medicine, Denver, CO, Dr. Yochum can be reached at 1-303-940-9400 or by e-mail at [email protected] Dr. Alicia M. Yochum is a third generation chiropractor and 2011 Suma Cum Laude Graduate of Logan College of Chiropractic, as well as a Registered Xurse. She is in a Radiology residency at Logan C Allege in St. Louis, MO. She can be reached at alicia.yochumd, gmail.com.