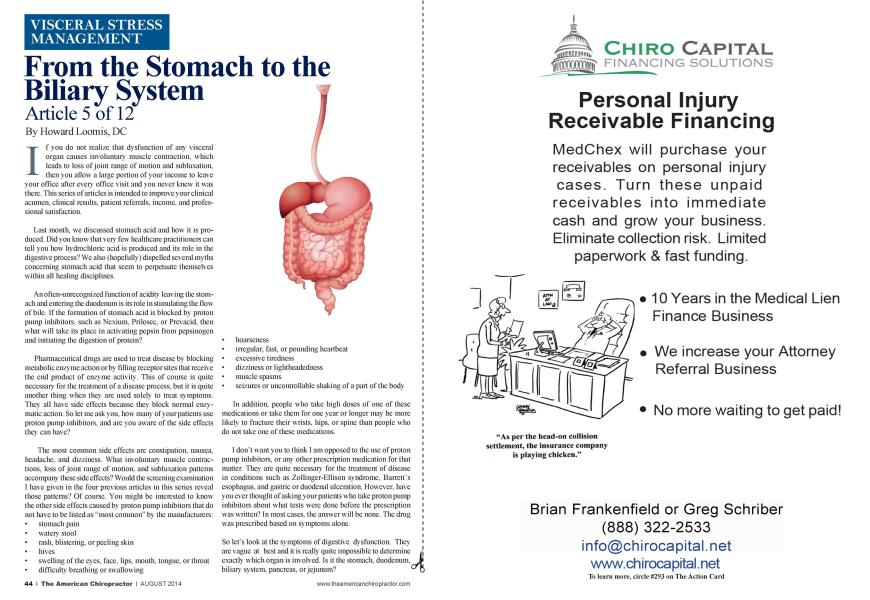
I f you do not realize that dysfunction of any visceral organ causes involuntary muscle contraction, which leads to loss of joint range of motion and subluxation. then you allow a large portion of your income to leave your office after every office visit and you never knew it was there. This series of articles is intended to improve your clinical acumen, clinical results, patient referrals, income, and professional satisfaction. Last month, we discussed stomach acid and how it is produced. Did you know tliat very few healthcare practitioners can tell you how hydrochloric acid is produced and its role in the digestive process? We also (hopefully) dispelled several myths concerning stomach acid that seem to perpetuate themselves within all healing disciplines. An often-unrecognized function of acidity leaving the stomach and entering the duodenum is its role in stimulating the flow of bile. If the formation of stomach acid is blocked by proton pump inhibitors, such as Ncxium. Priloscc. or Prcvacid. then what will take its place in activating pepsin from pepsinogen and initiating the digestion of protein? Pharmaceutical dmgs are used to treat disease by blocking metabolic enzyme action or by filling receptor sites that receive the end product of enzyme activity. This of course is quite necessary for the treatment of a disease process, but it is quite another thing when they are used solely to treat symptoms. They all have side effects because they block normal enzymatic action. So let me ask you. how many of your patients use proton pump inhibitors, and are you aware of the side effects they can have? The most common side effects are constipation, nausea, headache, and dizziness. What involuntary muscle contractions, loss of joint range of motion, and subluxation patterns accompany these side effects? Would the screening examination I have given in the four previous articles in this scries reveal those patterns? Of course. You might be interested to know the other side effects caused by proton pump inhibitors that do not have to be listed as "most common" by the manufacturers: stomach pain watery stool rash, blistering, or peeling skin hives swelling of the eyes. face. lips, mouth, tongue, or throat difficulty breathing or swallow ing hoarseness irregular, fast, or pounding heartbeat excessive tiredness dizziness or lightheadedness muscle spasms seizures or uncontrollable shaking of a part of the body In additioa people who take high doses of one of these medications or take them for one year or longer may be more likely to fracture their w rists. hips, or spine than people who do not take one of these medications. I don't want you to think I am opposed to the use of proton pump inhibitors, or any other prescription medication for that matter. They are quite necessary for the treatment of disease in conditions such as Zollinger-Ellison syndrome. Barrett's esophagus, and gastric or duodenal ulccration. However, have you ever thought of asking your patients who take proton pump inhibitors about what tests were done before the prescription was written? In most cases, the answer will be none. The drug was prescribed based on symptoms alone. So let's look at the symptoms of digestive dysfunction. They are vague at best and it is really quite impossible to determine exactly which organ is involved. Is it the stomach, duodenum, biliary system, pancreas, or jejunum? *■ Whatever the cause, it has led to the development of a multibillion-dollar industry, which includes not only prescription dmgs. but also over-the-counter sale of antacids and proton pump inhibitors. The problem with establishing a proper diagnosis is identifying which compromised organ is responsible for the following symptoms: Frequent Bitter Taste in Mouth History of Chronic Indigestion Loss of appetite, especially for meat Intolerance of fats and spicy foods Lower bowel gas, unaware of what foods cause the problem Frequent heartburn or indigestion with nausea and discomfort Undigested food, capsules, or tablets found in the stool Acid reflux after eating Unusual fullness after eating Stomach discomfort that is relieved by eating History of chronic gas, bloating, and distention Craving or thirst for cold liquids or foods Frequent abdominal cramping or discomfort after eating My point is that those who can accurately determine the cause of these symptoms and have a specific remedy available for restoring normal digestion instead of blocking digestion should be able to establish themselves as specialists in what apparently is an incredibly lucrative field. Besides, what normal body function must now compensate for an incompetent digestive system? The immune system, of course. Imagine your potential by specializing in this cause-and-effect area. So now we'll transition to the bilian system. The digestion of fat in the small intestine requires special processes to emulsify (degrease) fat molecules because fat is not soluble in water. This is caused by a group of detergent molecules known as bile salts, which are secreted by the liver into the bile ducts, then move on to join the pancreatic duct, and ultimately empty into the duodenum. All food high in fat must be emulsified. Bile does not contain any digestive enzymes. Bile is simply a degrcascr. Foods such as peanut butter and salad dressings are difficult to digest because of their oil content. Enzymes cannot penetrate the oil to digest the food unless the oil is degreased. Bile is necessary to expose the bonds within the food that the enzymes need to break. This is an important step in the digestive process. A large amount of gas will be formed if the action of bile is not adequate. Between meals, secreted bile is stored underneath the liver in a small sac known as the gallbladder, which concentrates the bile by absorbing salts and water. During a meal, the gallbladder contracts and a concentrated solution of bile is released into the small intestine. The presence of sodium and water added to the bile to neutralize stomach acid is equally important. When there is an insufficient amount of acid coming from the stomach, sodium and water arc extracted from the bile and put back into the blood. For this reason, gallbladder problems and stomach acid deficiencies are often synonymous. It is important to remember that predigestion of protein in the stomach by food enzymes creates acidity by breaking the amino acid bonds and releasing acid molecules, thus improving the flow of bile. When water and sodium arc rcabsorbed from the bile into the blood, the bile is thickened and its flow is very sluggish. This allows the formation of gallstones. They grow very slowly, but the symptoms of gas. bloating, pain, and constipation gradually become overwhelming. Eventually, the gallbladder is removed to correct the symptoms of gas. indigestion, and pain. When this is done, the surgeon simply makes a direct connection from the gallbladder to the pancreatic duct. The bile continues to drip constantly from the liver, and the body actually creates another small pouch. Even though the gallbladder is gone, the bile keeps coining and the hormone released by the wall of the small intestine keeps stimulating for its release. Nothing changes, except for the alleviation of the symptoms. The patient feels much better, but the bile is still too thick. More stones will form, and the symptoms usually come back in about two or three vcars. Dr. Howard Loomis has an extensive background in enzymes and enzyme supplements. He is the founder and president of Enzyme 1'bmiulationsX, Inc. His knowledge of physiology, biochemistry, and enzymology has made him a .sought-after .speaker and a pmlific writer. Dr. Loomi.s published ENZYMKS: The Kev to I Iealth in 1999. (intact info: 6421 Hnterprise Ixme, Madison, WI 53719, [email protected]