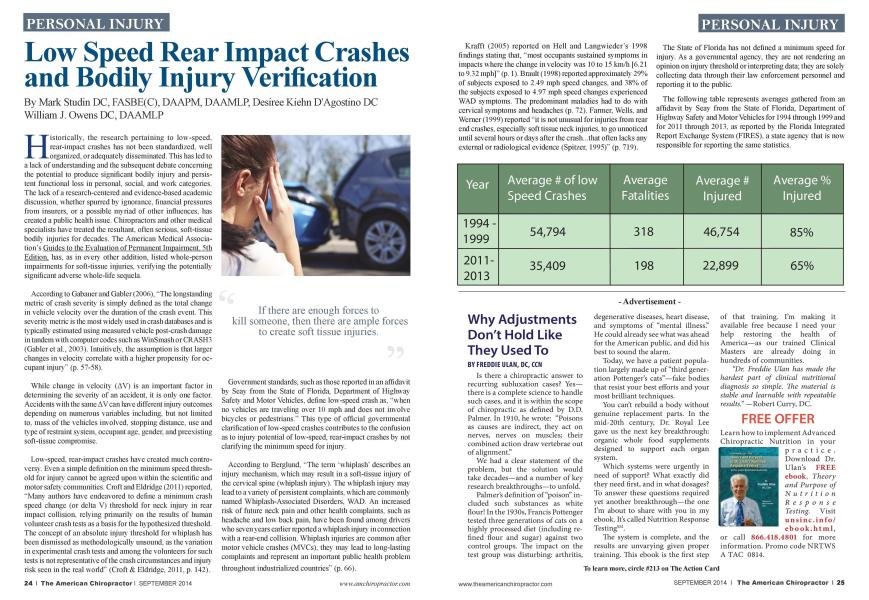
Historically, the research pertaining to low-speed, rear-impact crashes has not been standardized, well organized, or adequately disseminated. This has led to a lack of understanding and the subsequent debate concerning the potential to produce significant bodily injury and persistent functional loss in personal, social, and work categories. The lack of a research-centered and evidence-based academic discussion, whether spurred by ignorance, financial pressures from insurers, or a possible myriad of other influences, has created a public health issue. Chiropractors and other medical specialists have treated the resultant, often serious, soft-tissue bodily injuries for decades. The American Medical Association's Guides to the Evaluation of Permanent Impairment. 5th Edition, lias, as in even' other addition, listed whole-person impairments for soft-tissue injuries, verifying the potentially significant adverse whole-life sequela. According to Gabaucrand Gablcr(2006). "The longstanding metric of crash severity is simply defined as the total change in vehicle velocity over the duration of the crash event. This severity metric is the most widely used in crash databases and is typically estimated using measured vehicle post-crash damage in tandem with computer codes such as WinSmash or CR ASH3 (Gablcrct al.. 2003). Intuitively, the assumption is that larger changes in velocity correlate with a higher propensity for occupant injury" (p. 57-58). While change in velocity (AV) is an important factor in determining the severity of an accident, it is only one factor. Accidents with the same AV can have different injury outcomes depending on numerous variables including, but not limited to. mass of the vehicles involved, stopping distance, use and type of restraint system, occupant age. gender, and preexisting soft-tissue compromise. Low -speed, rear-impact crashes have created much controversy. Even a simple definition on the minimum speed threshold for injury cannot be agreed upon within the scientific and motor safety communities. Croft and Eldridgc (2011) reported. "Main authors have endeavored to define a minimum crash speed change (or delta V) threshold for neck injury in rear impact collision, relying primarily on the results of human volunteer crash tests as a basis for the hypothesized threshold. The concept of an absolute injury threshold for whiplash has been dismissed as methodologically unsound, as the variation in experimental crash tests and among the volunteers for such tests is not representative of the crash circumstances and injury risk seen in the real world" (Croft & Eldridgc. 2011. p. 142). Government standards, such as those reported in an affidavit by Scay from the State of Florida. Department of Highway Safety and Motor Vehicles, define low-speed crash as. "when no vehicles are traveling over 10 mph and does not involve bicycles or pedestrians." This type of official governmental clarification of low-speed crashes contributes to the confusion as to injury potential of low-speed, rear-impact crashes by not clarifying the minimum speed for injury. According to Bcrglund. "The term whiplash" describes an injury mechanism, which may result in a soft-tissue injury of the cervical spine (whiplash injury). The whiplash injury may lead to a variety of persistent complaints, which arc commonly named Whiplash-Associated Disorders. WAD. An increased risk of future neck pain and other health complaints, such as headache and low back pain, have been found among drivers who seven years earlier reported a whiplash injury in connection with a rear-end collision. Whiplash injuries arc common after motor vehicle crashes (MVCs). they may lead to long-lasting complaints and represent an important public health problem throughout industrialized countries" (p. 66). Krafft (2005) reported on Hell and Langwieder's 1998 findings stating that, "most occupants sustained symptoms in impacts where the change in velocity was 10 to 15 km/h [6.21 to 9.32 mph|" (p. 1). Brault (1998) reported approximately 29% of subjects exposed to 2.49 mph speed changes, and 38% of the subjects exposed to 4.97 mph speed changes experienced WAD symptoms. The predominant maladies had to do with cervical symptoms and headaches (p. 72). Fanner. Wells, and Werner (1999) reported "it is not unusual for injuries from rear end crashes, especially soft tissue neck injuries, to go unnoticed until several hours or days after the crash...that often lacks any external or radiological evidence (Spitzer. 1995)" (p. 719). The State of Florida has not defined a minimum speed for injury. As a governmental agency, they arc not rendering an opinion on injury threshold or interpreting data: they arc solely collecting data through their law enforcement personnel and reporting it to the public. The following table represents averages gathered from an affidavit by Scay from the State of Florida. Department of Highway Safety and Motor Vehicles for 1994 through 1999 and for 2011 through 2013. as reported by the Florida Integrated Report Exchange System (FIRES), a state agency that is now responsible for reporting the same statistics. Although the criterion for data collection may have changed over the years, the above table indicates that vehicles arc getting safer at low speeds as time progresses. Currently, according to ConsunicrRcports.org. as of 2010. the Insurance Institute for Highway Safety raised the minimum speed for crash worthiness to 40 mph in a frontal collision. This indicates that vehicle chassis have to be much more rigid, thereby sacrificing safety at low speeds. The Instituc's standard for low speed, rear-end crashes is a stationary car being struck by a target car of the same weight at 20 mph. The only solution the Insurance Institute offers for occupant safety at low speeds is higher headrests positioned closer to the head, with no further testing currently reported. According to Hijoka. Narusaw a. and Nakamura (2001). occupants in no-damage crashes suffer almost double the number of injuries of those in crashes where there was "total destruction" of the vehicle. The study revealed that when there was slight damage to the car. damage to the bumper, one-third of the car was damaged, or one-half of the car was damaged, occupants all had significantly more injuries than when there was total destruction of the automobile. When there was slight damage to the bumper, it was reported that almost every occupant was injured. The graph below is a visual representation of the statistics provided in the article: The rationale for a significant number of bodily injuries with little or no damage to the target car is explained by "crumple zones." As the car deforms and energy is transferred, we must take into consideration Newton's first law where energy can neither be created nor destroyed. When a crumple zone deforms, energy is released in the form of heat and sound, and the vehicle stopping time is elongated. This, in turn, lowers the amount of force transferred from the bullet car to the target car and ultimately to the occupant. The above graph verifies that more people arc injured when the car is not deformed due to reasons such as a stiffer chassis, which arc designed to protect the occupant at higher speeds resulting in safety at lower speeds being sacrificed. Although it lias been argued for years that occupants cannot be injured at low speeds, an opinion that has been seemingly supported with an intuitive conclusion that if the car is not damaged then the person cannot be injured, the previous graph verifies that occupants are injured at low speeds. In addition, according to the Florida statistics, many have died. The Hijoka graph validates the statistics cited earlier, along with main other articles through the years that have reported that occupants of vehicles involved in a low -speed crash can sustain serious bodily injury even in the absence of vehicle damage. The most obvious statistic is one regarding fatalities. There has consistently been a significant number of deaths reported over the past two decades by the State of Florida in low -speed crashes. Those arguing that it is not possible for injuries to be caused at low speeds can no longer overlook the fact that people arc dying in these types of collisions. If there arc enough forces to kill someone, then there arc ample forces to create soft-tissue injuries. These types of injuries can be documented through x-rays and x-ray digitizing along with MRI and CAT scans. Clinical Comment: Determining causality is a critical component in concluding an accurate diagnosis, prognosis, and treatment plan. The vector of impact along with the amount of force will help direct the trauma-trained practitioner to consider the appropriate soft tissue. osseous, or neurological element that lias potentially been injured. Therefore, it is critical for the practitioner to have advanced training in being able to conclusively diagnose his or her patients. References: I. Coccliiarella I... &■ Anderson, G (2001). Guides to the Evaluation of Permanent Impairment, 5th Edition. (liicago, IL: A.\LI Press. Gahauer D../.. & Gabler, H. C. (2006). Comparison of delta-v and oc cupant impact wlocity crash severity metrics using event data recorders. An imal Proceedings. Association for the Advancement of Automotive \ ledicine, 50. 57 71. Croft. A. C. cf- Eldndge. T. R (2011). Human subject rear passenger symptom ivsponse to frontal car-to-car low-speed crasli tests. Journal qf( lii- ropracticS ledicine. 10(3). 141-146. Sea}'. .\1.J. (2000. July 11). /Statistics obtained Florida traffic eras/; re ports/. 1,'npublishedrawdala. (Availablefrom the State oj 'Florida Department oflligliwas ■ Safety • andS lotor I eludes) lierglund. A..AIjredsson I... Jensen I.. Boclin L. & NygrenA. (2003). Oc cupant- and crash-related factors associated with Ok risk of whiplash injury. Annuls of Epidemiology. 13(1), 66-72. Kraf/l. S1.. Kullgren. A.. \ him, S, & Ydenius, A. (2005). Iiifhience ofcrasli severity on various whiplasli injury symptoms: A study based on real-life rear- end crashes witli recorded crash pulses. Paper presented at the 19th Interna tional Teclmical C Conference on Fjilianced Safety of I eludes. U ashington IX". Brault, J. II. II lieeler. J. It Siegmund. G. P. & Braull. E J. (1998). C lini- cal response of human subjects to rear-end automobile collisions. Archives of Physical Medicine and Rehabilitation. 79(1). 72 W. Farmer. C \L IVells.J A'.. cC- Werner. J. V. (1999). Relanowiup of head restraint positiaiingto driverneck injury in rear-endcrasties. AccidentAnalysis and Prevention. 31(6). 719-728. C 'onsumer Reports.org (2014). Crash test 101. How crasli worthiness is measured and how crasli ratings can he/pyvu choose your next car. Retrieved June 19. 2014. from blip: www.consumerreports. orgcro2011 08 crash- test-101 index.htm 10. Hi/oka. A.. Xarusawa. K.. &■ Xakamura. T. (2001). Risk Factors for long-term treatment of whiplash in Japan: Analysis of400 cases. Archives of Orthopedic and Trauma Surgery, 121(9), 490493. Dr. Mark Sludin is an adjunct assistant professor in clinical sciences at the University Of Bridgeport College Of Chiropractic r for the State of New York at Buffalo, School of Medicine and Biomedical Sciences. He can be reached al DrMark(a)AcademyofChiropractic.com or at 631-786-4253. Dr. Desiree Kiehn D 'Agostino graduated Summa Cum Laucle from Western Slates Chiropractic College. She is certified in MRI Spinal interpretation and practices evidenced based care treating trauma cases in Boston, Massachusetts. Dr. Owens presently has a large medical referral practice and has successfully integrated research, diagnostic and reporting protocols into communicating with the medical profession. He can be reached at 716.228.3847.