ANATOMY IN ACTION SERIES: Torticollis
Educational articles designed to help CAs understand the underlying anatomy and physiology of conditions presenting to the chiropractic office.
Laurie Mueller
What is Torticollis?
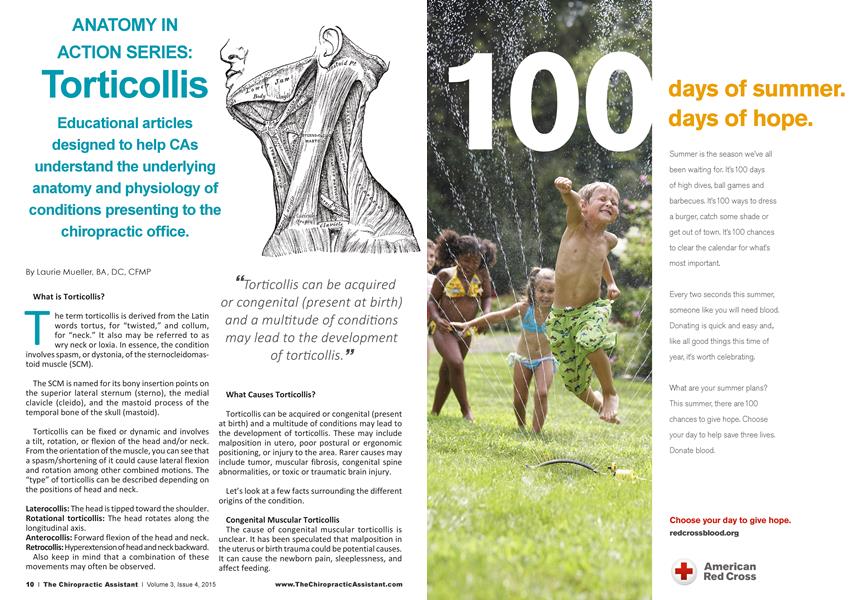
The term torticollis is derived from the Latin words tortus, for "twisted," and collum, for "neck." It also may be referred to as wry neck or loxia. In essence, the condition involves spasm, or dystonia, of the sternocleidomastoid muscle (SCM).
The SCM is named for its bony insertion points on the superior lateral sternum (sterno), the medial clavicle (cleido), and the mastoid process of the temporal bone of the skull (mastoid).
Torticollis can be fixed or dynamic and involves a tilt, rotation, or flexion of the head and/or neck. From the orientation of the muscle, you can see that a spasm/shortening of it could cause lateral flexion and rotation among other combined motions. The "type" of torticollis can be described depending on the positions of head and neck.
Laterocollis: The head is tipped toward the shoulder. Rotational torticollis: The head rotates along the longitudinal axis.
Anterocollis: Forward flexion of the head and neck. Retrocollis: Hyperextension of head and neck backward.
Also keep in mind that a combination of these movements may often be observed.
“Torticollis can be acquired or congenital (present at birth) and a multitude of conditions may lead to the development of torticollis.
What Causes Torticollis?
Torticollis can be acquired or congenital (present at birth) and a multitude of conditions may lead to the development of torticollis. These may include malposition in utero, poor postural or ergonomic positioning, or injury to the area. Rarer causes may include tumor, muscular fibrosis, congenital spine abnormalities, or toxic or traumatic brain injury.
Let's look at a few facts surrounding the different origins of the condition.
Congenital Muscular Torticollis
The cause of congenital muscular torticollis is unclear. It has been speculated that malposition in the uterus or birth trauma could be potential causes. It can cause the newborn pain, sleeplessness, and affect feeding.
The reported incidence of congenital torticollis is 0.3 to 2.0%. Sometimes a mass, such as a sternocleidomastoid tumor, is noted in the affected muscle at the age of two to four weeks. Gradually it disappears, usually by the age of eight months, but the muscle can be left fibrotic.
Acquired Torticollis
A self-limiting, spontaneously occurring form of torticollis with one or more painful neck muscles is by far the most common cause of “stiff neck" and will pass spontaneously in one to four weeks. Usually the sternocleidomastoid muscle or the trapezius muscle is involved. Sometimes draughts, colds, or unusual postures are implicated; however, in many cases no clear cause is found. These episodes are commonly seen by physicians.
Noncongenital muscular torticollis may also, however, result from a variety of other less common issues, such as scarring or disease of cervical vertebrae, adenitis, tonsillitis, rheumatism, enlarged cervical glands, retropharyngeal abscess, cerebellar tumors, or certain drugs. It may be spasmodic (clonic) or permanent (tonic). The latter type may be due to Pott's disease (tuberculosis of the spine).
Spasmodic Torticollis
Spasmodic torticollis features recurrent but transient contraction of the muscles of the neck and especially of the sternocleidomastoid. Synonyms are “intermittent torticollis," “cervical dystonia," or “idiopathic cervical dystonia," depending on cause.
Acquired Torticollis in Infants
Infants often develop torticollis as a result of the amount of time they spend lying on their backs during the day in car seats, swings, bouncers, strollers, and on play mats. Infants with torticollis also tend to have a higher risk of plagiocephaly, or flat head syndrome. Most pediatricians recommend regular repositioning of a baby for healthy head and neck movement. Torticollis is almost always preventable in infants.
Diagnosis
Evaluation of a child with torticollis begins with taking a history to determine circumstances surrounding birth and any possibility of trauma or associated symptoms. Physical examination reveals decreased rotation and bending to the side opposite of the affected muscle. Some say that congenital cases more often involve the right side, but there is not complete agreement about this in published studies.
Evaluation should include a thorough neurologic examination and the possibility of any associated
Because the spasmed muscle can put stress on other muscles and joints and cause subluxations, chiropractic adjustments coupled with physiotherapies can promote a faster resolution
for the patient.99
conditions. Radiographs of the cervical spine should be obtained to rule out obvious bony abnormality, and MRI should be considered if there is concern about structural problems or other conditions.
Ruling out rarer, more menacing causes of the condition, such as tumor or bony abnormality, would need to be accomplished prior to treatment.
Management of Torticollis
Chiropractic can be extremely effective for this condition. Because the spasmed muscle can put stress on other muscles and joints and cause subluxations, chiropractic adjustments coupled with physiotherapies can promote a faster resolution for the patient.
Initially, the condition may be treated with physical therapies, such as stretching to release tightness, strengthening exercises to improve muscular balance, and handling (of infants) to stimulate symmetry. For adults, EMS or ultrasound may be beneficial in relaxing the muscle. For congenital muscular torticollis, a TOT collar is sometimes applied. About 5 to 10% of congenital muscular cases fail to respond to stretching and may require surgical release of the muscle.
From a psychological standpoint for patients and care-providers alike, it can be alarming to have a
patient in such a contorted position. As treatment progresses, it is very rewarding to watch the patient become more balanced and comfortable.
For DCs who utilize nutrition in their practices, they may also optto recommend vitamins/minerals or herbs known for supporting muscle function or relaxation of muscles. These may include but not be limited to calcium, magnesium, CoQlO, B6, D3, or plant-based products such as valerian root.
Education Fosters Understanding
An understanding of anatomy and clinical applicability helps all health-office employees better communicate with patients and provide care more safely. Online training programs in particular make high-quality training affordable and convenient and can be taken any time of day. At CCCAonline.com, learners can engage in a streamlined 24-hour training program that meets or exceeds FCLB guidelines in every area of study and fulfill the training requirements needed for the national examination!
DCs will often pay for their employees to train. Full price for this training is an affordable $339 for the entire 24-hour program. CCCAonline.com also has a special discount available for you! If you received this article through The American Chiropractor magazine, then use AMCHIRO as your discount code. When this code is entered during the registration process, it will automatically provide a $15 discount off the regular price of the program. This is the program that gives back to the profession.
Learners can expect text, images/schematics, dynamic video lectures, and robust, customized experiential interactivities in a thorough 19-module program. An extensive note-packet of nearly 200 pages also is included and can be downloaded, printed, and studied off-line. Learners work attheir own pace and can conveniently take programming around work hours to avoid disruption in the office. Questions? Visit our website or send us an e-mail at [email protected].
H Laurie Mueller, BA, DC, CFMP served in private practice in San Diego, California. She was the postgraduate director at Palmer College from 2000 to 2010; served as the ACC postgraduate subcommittee chair for six years; peer reviewed for the Research Agenda Conference; and wrote the informal role determination study that aided in the development of FCLB's guidelines for chiropractic assistants. Dr. Mueller currently works as a private eLearning consultant with a focus on healthcare topics andfunctional medicine through her company, Impact Writing Solutions, and its subsidiary, www.CCCAonline.com. She is a clinician, educator, and expert in online educational pedagogy.