Clinical Certainty and Interoception
PERSPECTIVE
This dual channel feedback can significantly enhance a practitioner's sense of clinical certainty.
Robert “Ric” Wiegand
DC
Exteroception and Interoception: Two Distinct Channels of Feedback Information
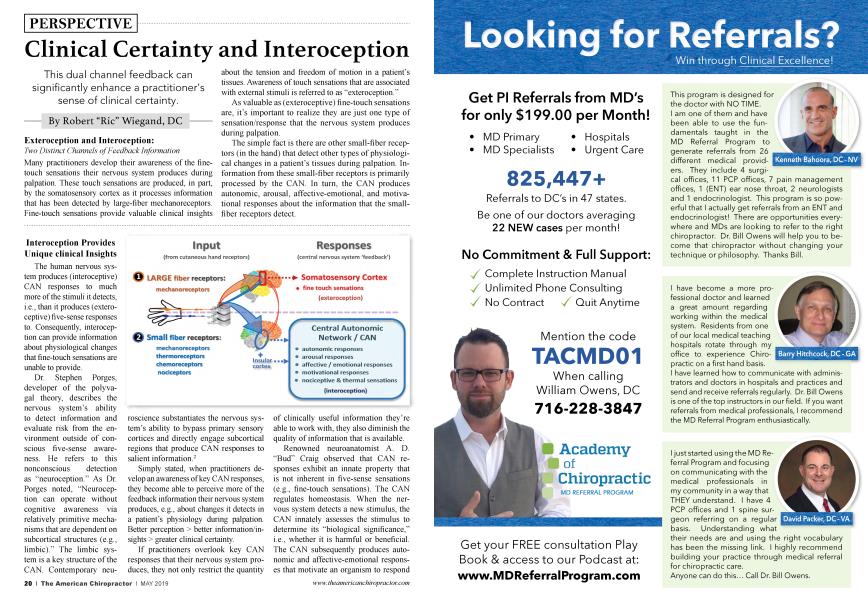
Many practitioners develop their awareness of the finetouch sensations their nervous system produces during palpation. These touch sensations are produced, in part, by the somatosensory cortex as it processes information that has been detected by large-fiber mechanoreceptors. Fine-touch sensations provide valuable clinical insights about the tension and freedom of motion in a patient’s tissues. Awareness of touch sensations that are associated with external stimuli is referred to as “exteroception.”
As valuable as (exteroceptive) fine-touch sensations are, it’s important to realize they are just one type of sensation/response that the nervous system produces during palpation.
The simple fact is there are other small-fiber receptors (in the hand) that detect other types of physiological changes in a patient’s tissues during palpation. Information from these small-fiber receptors is primarily processed by the CAN. In turn, the CAN produces autonomic, arousal, affective-emotional, and motivational responses about the information that the smallfiber receptors detect.
Interoception Provides Unique clinical Insights
The human nervous system produces (interoceptive) CAN responses to much more of the stimuli it detects, i.e., than it produces (exteroceptive) five-sense responses to. Consequently, interoception can provide information about physiological changes that fine-touch sensations are unable to provide.
Dr. Stephen Porges, developer of the polyvagal theory, describes the nervous system’s ability to detect information and evaluate risk from the environment outside of conscious five-sense awareness. He refers to this nonconscious detection as “neuroception.” As Dr. Porges noted, “Neuroception can operate without cognitive awareness via relatively primitive mechanisms that are dependent on subcortical structures (e.g., limbic).” The limbic system is a key structure of the CAN. Contemporary neuroscience substantiates the nervous system’s ability to bypass primary sensory cortices and directly engage subcortical regions that produce CAN responses to salient information.2
Simply stated, when practitioners develop an awareness of key CAN responses, they become able to perceive more of the feedback information their nervous system produces, e.g., about changes it detects in a patient’s physiology during palpation. Better perception > better information/insights > greater clinical certainty.
If practitioners overlook key CAN responses that their nervous system produces, they not only restrict the quantity of clinically useful information they’re able to work with, they also diminish the quality of information that is available.
Renowned neuroanatomist A. D. “Bud” Craig observed that CAN responses exhibit an innate property that is not inherent in five-sense sensations (e.g., fine-touch sensations). The CAN regulates homeostasis. When the nervous system detects a new stimulus, the CAN innately assesses the stimulus to determine its “biological significance,” i.e., whether it is harmful or beneficial. The CAN subsequently produces autonomic and affective-emotional responses that motivate an organism to respond in a homeostatically beneficial way.
Dr. Antonio Damasio, a neuroscientist who specializes in emotion research, notes that the human nervous system innately produces emotive responses for every perceptible stimulus.3 In effect, CAN responses intrinsically reflect the nervous system’s innate evaluation of the “goodness or badness” of a stimulus.
By comparison, the somatosensory cortex encodes qualities such as texture, tension, pressure, and vibration when it processes fine-touch sensations, but it does not encode a sense of the “significance” of finetouch sensations. Consequently, if practitioners only pay attention to fine-touch sensations, they must figure out the significance of the touch sensations cognitively, e.g., based on technique rules, experience, etc.
When practitioners develop interoception, they heighten their perception of their nervous system’s innate evaluation of the significance of stimuli that it detects. This enables a practitioner to “feel things out,” in addition to “figuring them out.” Interoceptive feedback can function as an “innate second opinion” that supports or qualifies information that is detected through exteroceptive feedback. This dual channel feedback can significantly enhance a practitioner’s sense of clinical certainty.
Why Not Take Greater Advantage of Innate Resources?
Given that the nervous system produces two channels of feedback during palpation, and each channel provides unique, clinically valuable information about a patient, a question that might be asked is why don’t more practitioners take advantage of both exteroceptive and interoceptive feedback when they palpate a patient?
One reason may have to do with outmoded beliefs about the role of emotions in the decision-making process. An outdated misconception is that emotions inherently interfere with rational analysis. Neuroscience no longer supports this idea. As noted by McGill University, “... we see that emotions, far from interfering with the making of rational decision in everyday life, actually constitute the essential condition for them.4
Another reason is simply that many practitioners never learned how to skillfully develop interoception. This is due, in part, to the fact that neuroscience only recently advanced to the point where it’s able to adequately explain how interception operates. Practitioners who have tried to develop interoception in the past had to go through an extended trial and error process, and relatively few succeeded. Consequently, interoception gained a reputation for being hard and time consuming to develop.
It’s not a matter of being hard; it’s a matter of knowing what to do. Information that is available now makes it possible for most practitioners to develop clinically useful interoception skills after a weekend of training.5
In closing, contemporary neuroscience supports the use of interoception in making clinical decisions. By developing interoceptive awareness, practitioners can get access to more information about dysfunctional changes that their nervous system detects in a patient’s physiology. This significantly contributes to greater clinical certainty and, in turn, to a more effective and enjoyable practice.
References:
1. Ann NY Acad Sci. 2018 Sep; 1428(1): 112-128. doi: 10.1111/nyas. 13915. Epub 2018 Jul 5. The neurobiology of interoception in health and disease. Quadt LI, Critchley HD 1,2, Garfinkel SN1,2. www.ncbi.nlm. nih.gov/pubmed/29974959
2. Bypassing Primary Sensory Cortices-A Direct Thalamocortical Pathway for Transmitting Salient Sensory Information M. Liang A. Mouraux G. D. Iannetti Cerebral Cortex, Volume 23, Issue 1,1 January 2013, Pages 1-11, academic.oup.com/cercor/article/23/1/1/327009
3. The Strange Order of Things: Life Feeling and the Making of Cultures; Damasio, A.;Pages 108 - 112
4. Neuropsychologists Show How Emotions Affect Cognition and Decision making thebrain.mcgill.ca/flash/ capsules/experience_bleu04.html
5. Observations of author attained via 35 years of interoceptive awareness coaching.
Dr. Robert "Ric" Wiegand is a cofounder of the Access Workshop, which offers a neuroscience-based approach for rapidly developing clinical interoception skills. He currently resides in Eugene, Oregon and can be reached at: