Energy Production and the Magic of Mitochondria
FUNCTIONAL MEDICINE
Laurie Mueller
DC, CFMP
ATP Is Essential to Life
The vast majority of our cellular functions require ATP in order to happen. This includes things such as synthesis of proteins, formation of cell walls and membranes, the movement of the cell, cell division, and the list goes on. ATP is often referred to as the “molecular unit of currency” for intracellular energy and use. At the core of energy production, we use the process of cellular respiration to exchange food particles of sugars/fats/proteins into our “energy currency.” This process mainly occurs through aerobic respiration within the mitochondria.
The average body contains about 250 grams of ATP at one time but turns over its own body weight equivalent in ATP each day.
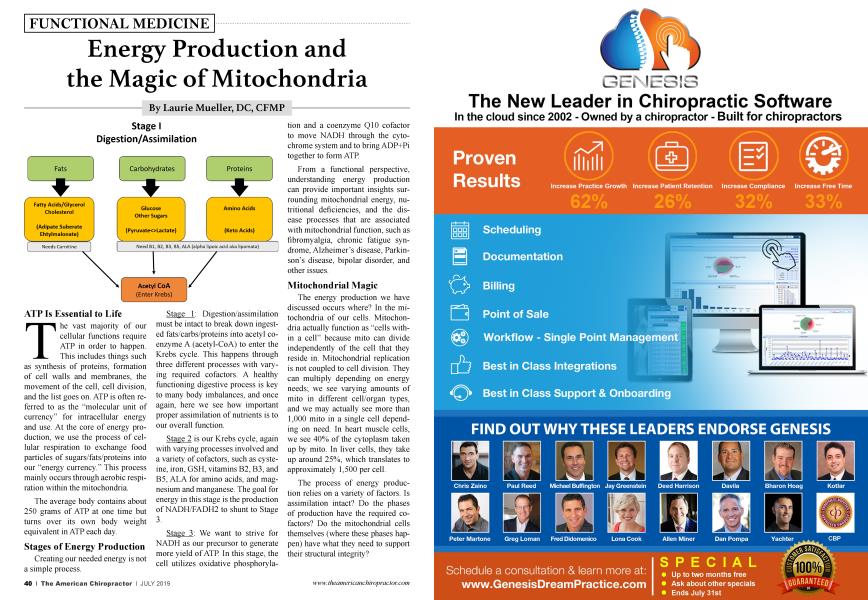
Stages of Energy Production
Creating our needed energy is not a simple process.
Stage 1: Digestion/assimilation must be intact to break down ingested fats/carbs/proteins into acetyl coenzyme A (acetyl-CoA) to enter the Krebs cycle. This happens through three different processes with varying required cofactors. A healthy functioning digestive process is key to many body imbalances, and once again, here we see how important proper assimilation of nutrients is to our overall function.
Stage 2 is our Krebs cycle, again with varying processes involved and a variety of cofactors, such as cysteine, iron, GSH, vitamins B2, B3, and B5, ALA for amino acids, and magnesium and manganese. The goal for energy in this stage is the production of NADH/FADH2 to shunt to Stage 3.
Stage 3: We want to strive for NADH as our precursor to generate more yield of ATP. In this stage, the cell utilizes oxidative phosphorylation and a coenzyme Q10 cofactor to move NADH through the cytochrome system and to bring ADP+Pi together to form ATP.
From a functional perspective, understanding energy production can provide important insights surrounding mitochondrial energy, nutritional deficiencies, and the disease processes that are associated with mitochondrial function, such as fibromyalgia, chronic fatigue syndrome, Alzheimer’s disease, Parkinson’s disease, bipolar disorder, and other issues.
Mitochondrial Magic
The energy production we have discussed occurs where? In the mitochondria of our cells. Mitochondria actually function as “cells within a cell” because mito can divide independently of the cell that they reside in. Mitochondrial replication is not coupled to cell division. They can multiply depending on energy needs; we see varying amounts of mito in different cell/organ types, and we may actually see more than 1,000 mito in a single cell depending on need. In heart muscle cells, we see 40% of the cytoplasm taken up by mito. In liver cells, they take up around 25%, which translates to approximately 1,500 per cell.
The process of energy production relies on a variety of factors. Is assimilation intact? Do the phases of production have the required cofactors? Do the mitochondrial cells themselves (where these phases happen) have what they need to support their structural integrity?
Take-Home Points: Are Your Patients Fatigued?
Patients may complain of being more tired, or they may have been diagnosed more formally with something such as chronic fatigue syndrome or fibromyalgia. If you think about it, nearly every disease process has fatigue as a symptom. An interesting note is that people suffering from Parkinson’s or Alzheimer’s disease have a much higher mitochondrial mutation rate than do healthy people, and research is starting to look at the function of the mitochondria in the implication of these and other disease processes.
Mitochondrial dysfunction can be inherent (inherited) or acquired. Typically, primary dysfunction results from inherited mtDNA mutation and is rare. Secondary dysfunction is becoming more recognized and results from the influence of external mechanisms, such as environmental or pharmacologic toxins, that can damage the mtDNA.
There are still those rare mitochondrial disease processes that are inherited (such as Leigh’s disease, Leber’s hereditary optic neuropathy [LOHN], or pyruvate dehydrogenase complex deficiency [PDCD]). However, our mainstream thinking is swiftly evolving to the current understanding and theory that mitochondrial dysfunction (found via secondary causation) could be at the core pathophysiology of many of our most common complex chronic diseases, which are the diseases showing up in our practices in increasing rates. Among those, we will find things such as insulin resistance, metabolic syndrome, nonalcoholic steatohepatitis (NASH), epilepsy, fatigue, fibromyalgia, neurodegeneration, multiple sclerosis, Huntington’s disease, Alzheimer’s disease, vascular inflammation, cardiovascular disease, etc.
Think about how patients’ bodies are functioning. Assess if their assimilation/digestive process is intact to provide a good foundation for Stage 1 energy production. Assess if they are ingesting the required cofactors for all stages of energy production and for mitochondrial cell health. Specifically for the mito cell, the outer membrane requires calcium and the inner membrane needs proteins and carnitine. Our Krebs cycle happens in the mitochondrial matrix, and all of our mito functions also require ATP.
Intact assimilation to drive our metabolic system and feed our mitochondria requires 13 vitamins, 11 minerals, eight amino acids, and two fatty acids.
Systemic inflammation also can have a profound effect on mitochondrial function. Patients need to stop eating sugar and simple carbohydrates, reduce free-radical build-up, and strive to reduce stress, which is a factor for most people.
You also will want to look at possible toxins that the patient can be exposed to that can affect mitochondrial function, which we are not able to include in this article.
Laurie Mueller, BA, DC, CFMP served in private practice in San Diego, California. She was the post-graduate director at Palmer College from 2000-2010; served as the ACC Post Graduate subcommittee chair for 6 years; and peer reviewed for the Research Agenda Conference. Dr. Mueller currently works as a private eLearning consultant with a focus on healthcare topics and functional medicine through her company, Impact Writing Solutions, LLC. She is a consultant, clinician, an educator and an expert in online educational pedagogy and is the founder of www.FxMedOnline.com. Explore more at FxMedOnline.com/ FxMedOnline.myicourse.com.TAC readers can also enjoy $10 off their first registration bundle by utilizing TAC's exclusive discount code at the time of purchase— TACFXMED.
References:
1. Bender DA, Mayes PA. Chapter 18. Glycolysis and the Oxidation of Pyruvate. In: Bender DA, Botham KM, Weil PA, Kennedy PJ, Murray RK, Rodwell VW, eds. Harper ⅛ Illustrated Biochemistry. 29th ed. New York: McGraw-Hill; 2011. Accessed May 14, 2013.
2. http://www.sciencedirect. com science article pii S221464741400004X Association of mitochondrial dysfunction and fatigue: A review of the literature Kristin Fillera, c, , , Debra Lyonb, , et al. BBA Clinical Volume 1, June 2014, Pg 12-23.
3. https://www. ncbi. nlm.nih.gov pmc articles PMC1762815/Nat Rev Genet. Author manuscript; available in PMC 2007 Jan 4.Published in final edited form as: Nat Rev Genet. 2005 May; 6(5): 389-402. doi: 10.1038/nrgl606PMCID: PMC1762815EMSID: UKMS5811 Mitochondrial DNA mutations in human disease Robert W. Taylor and Doug M. Turnbull
4. https://www. ncbi. nlm.nih.gov pmc articles PMC3422768/ Immunol Rev. Author manuscript; available in PMC 2013 Sep 1. Published in final edited form as.Tmmunol Rev. 2012 Sep; 249(1): 218-238. doi: 10. Ill 1/j. 1600065X2012.01151. xPMCID: PMC3422768NIHMSID: NIHMS383376 The inflammation highway: Metabolism accelerates inflammatory traffic in obesity Amy R. Johnson, J. Justin Milner, and Liza Makowski