Forced Evolution in the Electronic Age
TECHNIQUE
Alan Creed
DC
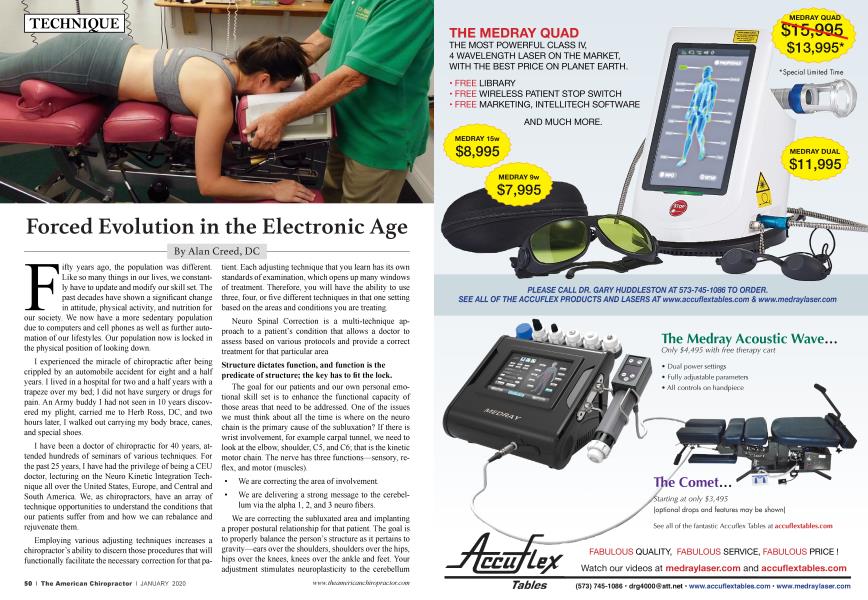
Fifty years ago, the population was different. Like so many things in our lives, we constantly have to update and modify our skill set. The past decades have shown a significant change in attitude, physical activity, and nutrition for our society. We now have a more sedentary population due to computers and cell phones as well as further automation of our lifestyles. Our population now is locked in the physical position of looking down.
I experienced the miracle of chiropractic after being crippled by an automobile accident for eight and a half years. I lived in a hospital for two and a half years with a trapeze over my bed; I did not have surgery or drugs for pain. An Army buddy I had not seen in 10 years discovered my plight, carried me to Herb Ross, DC, and two hours later, I walked out carrying my body brace, canes, and special shoes.
I have been a doctor of chiropractic for 40 years, attended hundreds of seminars of various techniques. For the past 25 years, I have had the privilege of being a CEU doctor, lecturing on the Neuro Kinetic Integration Technique all over the United States, Europe, and Central and South America. We, as chiropractors, have an array of technique opportunities to understand the conditions that our patients suffer from and how we can rebalance and rejuvenate them.
Employing various adjusting techniques increases a chiropractor’s ability to discern those procedures that will functionally facilitate the necessary correction for that patient. Each adjusting technique that you learn has its own standards of examination, which opens up many windows of treatment. Therefore, you will have the ability to use three, four, or five different techniques in that one setting based on the areas and conditions you are treating.
Neuro Spinal Correction is a multi-technique approach to a patient’s condition that allows a doctor to assess based on various protocols and provide a correct treatment for that particular area
Structure dictates function, and function is the predicate of structure; the key has to fit the lock.
The goal for our patients and our own personal emotional skill set is to enhance the functional capacity of those areas that need to be addressed. One of the issues we must think about all the time is where on the neuro chain is the primary cause of the subluxation? If there is wrist involvement, for example carpal tunnel, we need to look at the elbow, shoulder, C5, and C6; that is the kinetic motor chain. The nerve has three functions—sensory, reflex, and motor (muscles).
• We are correcting the area of involvement.
• We are delivering a strong message to the cerebellum via the alpha 1, 2, and 3 neuro fibers.
We are correcting the subluxated area and implanting a proper postural relationship for that patient. The goal is to properly balance the person’s structure as it pertains to gravity—ears over the shoulders, shoulders over the hips, hips over the knees, knees over the ankle and feet. Your adjustment stimulates neuroplasticity to the cerebellum and the frontal lobe of the brain. Through our years of practice, as many of us have found, the emotional state of our patients changes for the better as they participate in care.
Multi-Technique Approach
We have a myriad of choices with adjusting technique and styles. When we adjust a patient we use our hands along with the many adjusting devices provided to us through various techniques, such as SOT blocks, Thompson table drops, manual and electrical adjusting instruments, and Cox Flexion distraction table. Each technique has its own advantages. These instruments are an extension of our brains. For example, by employing the bifurcated head attachment on an electrical or manual instrument, you are able to capture the subluxated area in motion where it is locked. A cervical coupling lock can be unlocked very quickly to bring the head straight and level again with increased range of motion. The same procedure during a rotation of the thoracolumbar spine (i.e., T 12/Ll) can also be unlocked, which will significantly increase motion of the spine and diminish pain and discomfort in the lumbar. This type of adjustment on T 12/Ll can be performed manually in a side posture or sitting thoracolumbar Logan style. Employing instruments will simplify and aid in the complexities of an adjustment.
The goal in adjusting is to reset the integrity of muscles that provide structural orientation for the gravitational pull on the patient’s posture.
Therefore, when we adjust, we are addressing bones, nerve, disc, and the biggest issue of all, facet plane orientation. The outcome is for a balanced body relationship to gravity whether standing, walking, or sitting.
The cascading effects of subluxation will manifest in multiple ways, such as pain, discomfort, and inability to perform activities. This affects other areas of the body due to aberrant positions, limited blood flow, and compressive irritation of the nerves.
Cascading Effects of Anterior Head Translation
Patients presenting with an anterior head translation and kyphosis in the thoracic region will have lumbar and cervical pain. Sensory motor amnesia is created by a constant firing of various muscle groups due to gravity, nerve irritation, and habitual positions. This condition is caused by anterior head translation. The muscles are continually firing to support the thoracic cervical column from the gravitational pull that has been enhanced due to aberrant positions. As this is an ever-constant situation, the brain loses control, and our adjustments are the key to waking up the neuro kinetic chain.
Anterior head translation affects the heart and lungs due to T1 and T2 being compressed. Addressing the kyphosis will facilitate the nerve flow to the stomach, pancreas, gallbladder, adrenal cortex, spleen, stomach, and liver. The kyphosis that stands at T6/T7/T8 with an increased forward curved angle further irritates the lower back because the loads are now greater due to more flexion in the thoracic spine.
Neuro Kinetic Integration Technique provides for a global approach of the neuro spinal correction with the postural concept; allowing for a proper resetting of the proprioceptors as to the supporting musculature. Transmitting proper input in this style of adjusting will reduce gravitational pulls as well as increase muscle coordination and function. For example, in regard to anterior head translation, the head is anterior to the frame of the body, and in many cases, the head is locked in flexion. As it pertains to balance and gait stability, proprioceptors are directly communicating with the vestibular system, i.e., the muscles in the inner ears. If the head is forward, the cerebellum will fire the wrong muscles at the wrong time, leading to dizziness, stiffness, spasm, muscle tenderness, lower back pain, digestive upset, and extremity issues.
When correcting a subluxated area, it is incumbent for the doctor to have the patient in a proper position for the adjustment. To address a kyphosis, lay the patient prone on the table and elevate the head as high as can be with comfort, adding SOT blocks to balance the hips. We want to mirror image communicating to the brain where the head should be.
As an example, there are three choices when addressing the kyphosis:
1. Carver bridge or anterior thoracic move, manual by hands
2. Carver bridge by hand with thoracic drop concurrent done multiple times
3. Electrical instrument moving up and down the spine with the bifurcated headpiece adjusting the areas of enhanced kyphosis. This type of adjustment will provide a more correct structural posture for the patient, reducing gravitational pull because the head and thoracic region have been adjusted along with the low back.
We have patients with low back issues that are perpetuated by the upper cervical. This scenario further irritates the hips, legs, and feet, which is the body’s foundation. Greater loads are put more on the anterior portion of the feet due to anterior head translation. In order for the brain to hold the adjustment, we look at the mechanics of the feet as well; our patients must have shoes that will provide proper support. Due to poor construction of shoes, patients are walking in with narrow shoes as well as high heels, which place more pressure demands on the forefoot, especially creating prolapsing of the metatarsal heads.
We need to educate our patients on what a proper-titting shoe is and how it will benefit their structure by giving correct proprioceptive information to the cerebellum for position and space. A proper shoe has an arch support and at least half an inch of room in the toe box for the foot to spread properly as someone walks in it.
The world has changed; people want faster results to resume their lifestyles. We are the model, and we have to know as many different techniques as possible to facilitate changes that are dramatic to our patients. To paraphrase Abraham Lincoln, “If you only have a hammer, every condition is a nail.” Thomas Edison had a multitude of technicians working for him, which created an extraordinary amount of world inventions.
We are the “now”; we are the neuro structural engineers for our time.
Located in Miami, Dr. Alan Creed is a practicing chiropractic physician who is certified in acupuncture. Dr. Creed is a postgraduate professor of spinal biomechanics and neurophysiology, and a wellknown authority on integrating instrument adjusting in the chiropractic practice—ArthroStim, VibraCussor, drop table, SOT blocks, and spinal decompression. Dr. Creed is the innovator of the Neuro Kinetic Integration Technique and is an internationally known author, lecturer, and mentor of training manuals and videos for doctors. Dr. Creed's latest adjusting manual on Neuro Kinetic Integration Technique has been a bestseller in the profession.