Last month, my partner, Dr. Perry Bard, and I spent over an hour with Dr. Norman Shealy, MD, PhD, talking about spinal surgery, Non-Surgical Spinal Decompression (NSSD), his research, and different types of machines. His answers were exhilarating. Imagine a neurosurgeon, a former professor at Harvard Medical School, talking with us about sacral kinesiopathology and Failed Back Surgery Syndrome (FBSS). He told us he knew early on in his career that back surgery wasn’t the answer, which led him to find an alternative to surgery.
More than 500 papers of Dr. Shealy’s have been published. He is considered one of the most published and accomplished in his profession. He changed the face of decompression with his research. His work with other leading physicians led to the development of the fixed tower to isolate and treat specific segments. He was instrumental in treating patients from prone to supine. He was also germane in the research and further development of IDD therapy, utilizing a patented wavelength algorithm called oscillation to create imbibition. Dr. Shealy revolutionized NSSD, utilizing specific belting techniques, a sinusoidal algorithm, and the further development of the fixed tower, which he found necessary to isolate disc segments. Even today, he continues to study health and back pain at 88 years young. A true genius, Dr. Shealy says, “Any doctor doing decompression has an obligation to the patient, to their practice, to themselves to be nationally and university certified.”
Along with Dr. Shealy, another doctor was prompted by the poor success rate and high incidence of complications from spine surgery, and Non-Surgical Spinal Decompression was developed soon after that. In 1991, a medical researcher and Minister of Health Care for Canada, Dr. Allan Dyer, MD, PhD, created the first therapeutic device to mechanically reduce nerve compression. Combining his medical understanding with basic physics principles, Dr. Dyer reasoned that applying a sufficient axial load to the spine would create a vacuum in the disc that could reduce the protrusion of a herniated disc. It helped Dr. Dyer find relief from his back pain and was quickly embraced by the conservative healthcare community. Before his passing, we spoke often, and I learned so much from him.
Over the years, he and Dr. Shealy talked and often shared their thoughts. I am blessed to have worked with, been endorsed by, and to have spoken with these two great doctors on numerous occasions.
When Dr. Bard and I spoke with Dr. Shealy last month, we hung on to his every word. It was like talking to Thomas Edison about the light bulb. We were flattered when he passed the torch to us because we promised to continue our work. He was pleased and outwardly endorsed our work for both Disc Centers of America and the National Certification Program, which has now been taught at Parker University, National University, and Life University. His recognition of our work is the highlight of our professional careers.
Dr. Shealy also spoke with us about the dangers of pain and drug addiction. Did you know that 99% of oxycodone usage is in the U.S.? The cost of this medication first made national attention with Newsweek magazine’s article “The Price of Back Pain,” which stated, “Despite a growing array of sophisticated drugs, diagnostics, physical therapies, and surgical techniques, the millions of Americans battling back pain may not be any closer to getting that quick relief than they were 20 years ago.”
As the article points out, though, recent studies show even high-tech medical treatments rarely resolve back problems, while the prices charged for them continue to rise.
According to Newsweek, “In 2005 Americans spent $85.9 billion looking for relief from back and neck pain through surgery, doctor’s visits, X-rays, MRI scans, and medications, up from $52.1 billion in 1997.” However, the number of sufferers increased over that period; in 2005, 15% of U.S. adults reported back problems, compared with 12% in 1997.
In addition, a study in the Journal of the American Medical Association compared data from 3,179 adult patients who reported spine problems in 1997 to 3,187 who reported them in 2005. The research showed that annual medical costs rose from $4,700 per person to $6,100, adjusted for inflation. So more people are seeking treatment for back pain, and the price of treatment is increasing.
"...The cycling of the pressure produced by a specific algorithm helps create a pumping action that improves circulation and helps rehydrate the disc..."
In recognition of the impact that musculoskeletal disorders have on society, the United Nations and the World Health Organization designated 2000 to 2010 as the “Bone and Joint Decade.” They cited 10 million Americans disabled because of back pain. Those numbers have clearly risen since then.
Back and neck pain are among the leading causes of health issues facing people today. More than 10% of visits to primary care doctors are because of back or neck pain. The cost of such problems amounts to some $86 billion each year.
Over a quarter of patients with back pain complaints will have the same complaint again within a year. It is the most common cause of missed days of work in the U.S. Patients who are out of work because of back pain for six months or more rarely return to work. It remains the most expensive cause of work disability in the country.
The problem is not confined to the U.S. either. In Australia, it is the fastest-growing condition and accounts for over 50% of work loss and costs over $10 billion every year.
Dr. Shealy talked in detail about the utilization of drugs and adverse medical visits as leading causes of death in our country.
Non-Surgical Spinal Decompression (NSSD) machines are not the same as inversion or traction units. Dr. Shealy discussed this in detail and said, “Traction just doesn’t really work.” To learn more about this, read the Shealy-Borgmeyer study1.
Dr. Shealy does not like or believe in inversion systems. With inversion, a load-bearing traction force is generated by hanging from a person’s ankles or knees. Then there is the subjective angle—the only control over the force is the angle at which the patient hangs. The force is static unless you move. Studies from both Harvard University and the Mayo Clinic also disapprove of inversion.
Dr. Shealy stated that, with a true spinal decompression machine, the force is controlled and directed by utilizing specific algorithms and angles. The rate of application of pressure, the maximum and minimum levels of force, and the length of pressure application are all programmed into the machine. The cycling of the pressure produced by a specific algorithm helps create a pumping action that improves circulation and helps rehydrate the disc. It is particularly important with disc conditions since discs do not have a direct blood supply. We talked about the Boxell-Martin study5, which states that discs are active and have the ability to heal. In addition to being effective, spinal decompression is safe and pain-free. All decompression machines should be FDA-cleared and can be turned off by the patient if they experience any discomfort.
Spinal surgery often consists of two procedures performed at the same time—a procedure to remove the tissues causing the nerve impingement followed by spinal fusion. However, as Dr. Shealy stated, this should be the last resort, and up to 90% of all cases would do better with NSSD.
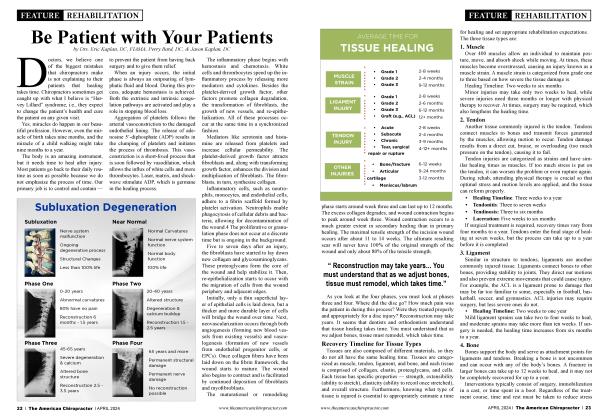
The most common types of decompressive surgeries are laminotomies and laminectomies. These procedures sound very similar because they both involve the lamina of your spine. Each vertebra in a patient’s spine has a lamina on either side of the posterior aspect, which creates a bony arch that encases the spinal cord. A laminectomy involves complete removal of this bony arch as the lamina is removed, whereas a laminotomy will only remove the portion of bone causing the nerve impingement.
The type of surgery a patient receives depends on the extent of nerve compression and if other procedures need to be completed. To perform both a laminectomy and a laminotomy, an incision is made at the vertebral level where the nerve compression occurs. The tissue is opened, cutting through skin and dissecting muscle to expose the bone of the spine. In a laminectomy, the spinous process and lamina are completely removed from the vertebra to relieve the pressure caused by these structures on the nerve roots or spinal cord. These bony structures can be seen below. The spinous process is a bony landmark that serves as a muscle attachment site, while the lamina forms the arch that covers the spinal cord. A laminotomy will keep some of those bony structures intact but will still require the removal of some of the lamina by cutting away the bone to decompress the nerve. That can lead to severe scar tissue formation and future nerve entrapment.
As we’ve learned, if those surgeries alone are not enough to completely decompress the nerve, the surgeon may elect to perform additional procedures before closing the initial entry incision. Depending on where the nerve compression occurred, it may call for a discectomy to remove part or all of a bulging/herniated disc. Finally, a foraminotomy may be performed to remove bone spurs or open the canals (foramen) where the nerve root exits the spine.
With a laminectomy, removing significant portions of bone creates the potential for instability in that region of the spine. In addition, some of the intrinsic muscles that are primary stabilizers of the spine attach directly onto portions of the removed vertebra, which makes the patient vulnerable to falls and severe Degenerative Joint Disease (DJD).
Remember, a surgeon has to cut through the paraspinal muscles to access the disc and lamina. Those muscles are responsible for helping to straighten the back, rotate, and keep the body upright. As a result, a laminectomy is often combined with a spinal fusion at that level, which requires the surgeon to drill screws into the vertebra above and below the affected level and connect them with steel rods.
Dr. Shealy discussed that the success rate was not good. He gave us so much material that we are excited to share at the National Certification Program in November. As stated by Dr. Shealy, it’s a doctor’s obligation to keep learning. He agreed with Dr. Bard and me on the importance of becoming a disc expert. A disc specialist needs to know everything about the anatomy and all procedures that are subsequent.
It is important to know that hardware is often required to maintain stability with surgery. That, in turn, creates a block of bones that can severely restrict normal ranges of motion. Even if the surgery is successful in reducing nerve compression, it comes at the cost of a permanent loss of normal movement and severe future scar tissue that can irritate the nerves. The result of this restriction can accelerate degeneration of the discs and joints bn above and below the fusion site, resulting in pain, inflammation, and, potentially, additional surgeries.
In closing, we talked in detail about the Shealy-Borgmeyer study1 that is often footnoted. The summary of it reads:
“We have compared the pain-relieving results of traditional mechanical traction (14 patients) with a more sophisticated device, which decompresses the lumbar spine, unloading of the facets (25 patients). The decompression system gave ‘good’ to ‘excellent’ relief in 86% of patients with RID and 75% of those with facet arthroses. The traction yielded no ‘excellent’ results in RID and only 50% ‘good’ to ‘excellent’ results in those with facet arthroses. These results are preliminary in nature. The procedures described have not been subjected to the scrutiny of review nor scientific controls. These patients will be followed for the next six months, at which time, outcome-based data can be reported. These preliminary findings are both enlightening and provocative.”
Dr. Shealy believes it is important to utilize research materials on the tables that you work with. I invite you to attend the National Certification Program on NSSD, which will be held this year on November 6-7 in Jupiter, Florida, sponsored by Life University for 12 CEU’s. Never-before-seen video clips of Dr. Shealy’s will be shown at this life-changing seminar.
Dr. Eric Kaplan and Dr. Perry Bard, are business partners of over 32 years. They have developed Disc Centers of America & Concierge Coaches, as well as the first and largest National Certification Program for Non-Surgical Spinal Decompression. Currently, they have over 150 clinics using their Disc Centers of America brand and lead ongoing success training events throughout the year. For more information see: www.thechiroevent.com, www.deco... or call 1-888-990-9660 to their Chiropractic Q&A Hotline.
References