IN LATE JULY 2025, A HEALTHY WOMAN IN HER 70s was diagnosed with a cervical mass measuring 1.5 cm. She had been referred for an ultrasound by her medical doctor due to symptoms of breakthrough bleeding.
The bleeding was thought to possibly be caused by fibroids and initiation of bioidentical hormone therapy earlier in the year (both progesterone and estrogen), but caution is always advised to rule out a cancerous mass. Four months later, by late November 2025, the mass had pretty much doubled in size to 2.9 cm.
Since the mass was vascular, it was explained that they could not do a biopsy and that the only way to tell if the mass was cancerous was to remove it. The first MD recommended a total hysterectomy. The second MD, an oncologist, was a little more conservative but still said that the only way to tell if it was cancerous was to remove the cervix.
This woman was urged by her holistic practitioner to lobby for time to reduce the size of the mass, which would prove it was not cancerous. The oncologist was willing to give it three weeks, but no more, because if it was cancer, it was risky to continue letting it grow.
Twenty-one days is not a lot of time to shrink a mass, but she was up to the challenge. She was put on a rigorous nutritional protocol that involved strict dietary restrictions of no sugar or alcohol, with limited carbohydrates.
Supplements included a lot of immune support, multivitamin and minerals, extra vitamin D (shown to be one of the best vitamins for fibroid support), vitamin K, vitamin C, etc., along with DIM and other nutrients to balance estrogen byproducts. However, since the most promising nutrient application seemed to be proteolytic enzymes, she was put on a very aggressive protocol of the enzymes.
As the author of this article, I can vouch for the efficacy of proteolytic enzymes. I wrote an article for The American Chiropractor in February 2002 on how I was able to overcome a ruptured disc at C-7 with enzymes when surgery seemed imminent, which results in a much weaker structure than healing naturally.
I had read several books about the benefits of proteolytic enzymes, which basically mop up the proteinaceous debris that initiates inflammation and used them in an aggressive protocol.1-2 I also knew that enzymes have been utilized for fibroid protocols.3 I used a combination of pancreatin, trypsin, chymotrypsin, pancrelipase, amylase, papain, and bromelain.
I took the enzymes three hours after my last meal, and took more the morning after, fasting until 2:00 p.m. After being bedridden for three weeks, I was able to experience a remarkable turnaround after 24 hours, and before the month was out, I was returning to the gym to lift light weights.
But enough about me, it looked as if an aggressive proteolytic enzyme protocol was warranted for this patient. “Lytic” refers to lysis, or cleaving, and proteolytic enzymes go after superfluous, unwanted tissue in the body, which is why enzymes are commonly used for support of fibroids.
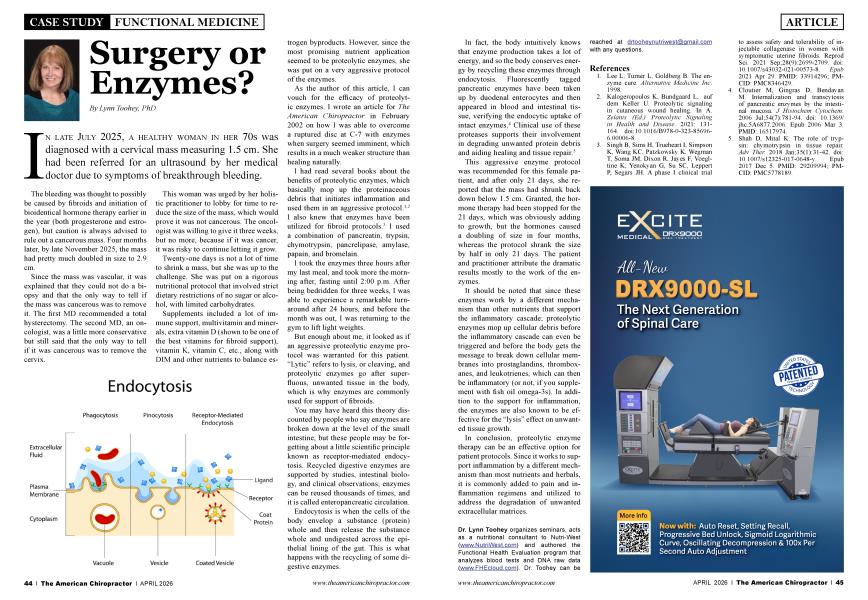
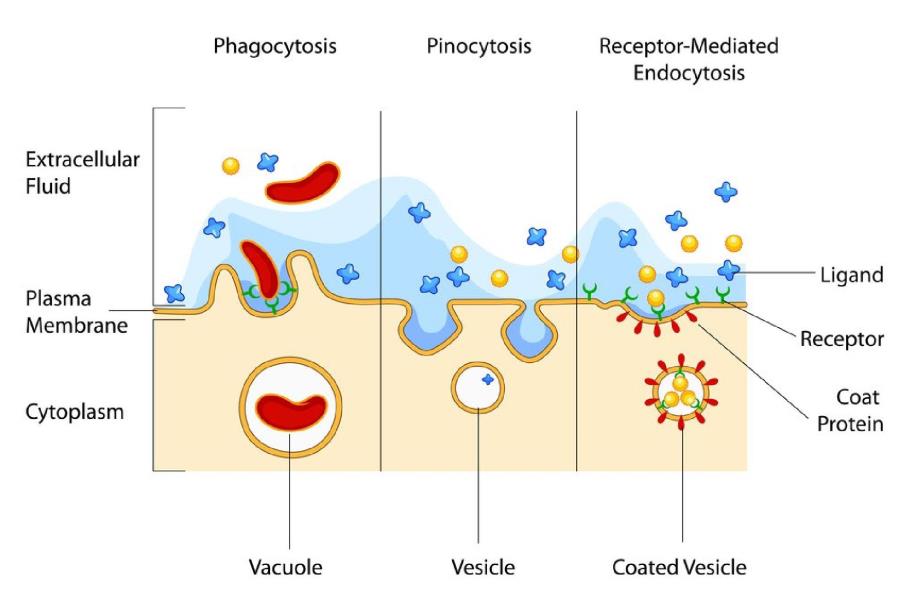
You may have heard this theory discounted by people who say enzymes are broken down at the level of the small intestine, but these people may be forgetting about a little scientific principle known as receptor-mediated endocytosis. Recycled digestive enzymes are supported by studies, intestinal biology, and clinical observations; enzymes can be reused thousands of times, and it is called enteropancreatic circulation.
Endocytosis is when the cells of the body envelop a substance (protein) whole and then release the substance whole and undigested across the epithelial lining of the gut. This is what happens with the recycling of some digestive enzymes.
In fact, the body intuitively knows that enzyme production takes a lot of energy, and so the body conserves energy by recycling these enzymes through endocytosis. Fluorescently tagged pancreatic enzymes have been taken up by duodenal enterocytes and then appeared in blood and intestinal tissue, verifying the endocytic uptake of intact enzymes.4 Clinical use of these proteases supports their involvement in degrading unwanted protein debris and aiding healing and tissue repair.5
This aggressive enzyme protocol was recommended for this female patient, and after only 21 days, she reported that the mass had shrunk back down below 1.5 cm. Granted, the hormone therapy had been stopped for the 21 days, which was obviously adding to growth, but the hormones caused a doubling of size in four months, whereas the protocol shrank the size by half in only 21 days. The patient and practitioner attribute the dramatic results mostly to the work of the enzymes.
It should be noted that since these enzymes work by a different mechanism than other nutrients that support the inflammatory cascade; proteolytic enzymes mop up cellular debris before the inflammatory cascade can even be triggered and before the body gets the message to break down cellular membranes into prostaglandins, thromboxanes, and leukotrienes, which can then be inflammatory (or not, if you supplement with fish oil omega-3s). In addition to the support for inflammation, the enzymes are also known to be effective for the “lysis” effect on unwanted tissue growth.
In conclusion, proteolytic enzyme therapy can be an effective option for patient protocols. Since it works to support inflammation by a different mechanism than most nutrients and herbals, it is commonly added to pain and inflammation regimens and utilized to address the degradation of unwanted extracellular matrices.

Dr. Lynn Toohey organizes seminars, acts as a nutritional consultant to Nutri-West (www.NutriWest.com) and authored the Functional Health Evaluation program that analyzes blood tests and DNA raw data (www.FHEcloud.com). Dr. Toohey can be reached at [email protected] with any questions.
1. Lee L, Turner L, Goldberg B. The enzyme cure. Alternative Medicine Inc. 1998.
2. Kalogeropoulos K, Bundgaard L, auf dem Keller U. Proteolytic signaling in cutaneous wound healing. In A. Zelanis (Ed.) Proteolytic Signaling in Health and Disease. 2021: 131164. doi: 10.1016/B978-0-323-856966.00006-8.
3. Singh B, Sims H, Trueheart I, Simpson K, Wang KC, Patzkowsky K, Wegman T, Soma JM, Dixon R, Jayes F, Voegltine K, Yenokyan G, Su SC, Leppert P, Segars JH. A phase I clinical trial
to assess safety and tolerability of injectable collagenase in women with symptomatic uterine fibroids. Reprod Sci. 2021 Sep;28(9):2699-2709. doi: 10.1007/s43032-021-00573-8. Epub 2021 Apr 29. PMID: 33914296; PMCID: PMC8346429.
4. Cloutier M, Gingras D, Bendayan M. Internalization and transcytosis of pancreatic enzymes by the intestinal mucosa. J Histochem Cytochem. 2006 Jul;54(7):781-94. doi: 10.1369/ jhc.5A6877.2006. Epub 2006 Mar 3. PMID: 16517974.
5. Shah D, Mital K. The role of trypsin: chymotrypsin in tissue repair. Adv Then 2018 Jan;35(l):31-42. doi: 10.1007/sl2325-017-0648-y. Epub 2017 Dec 5. PMID: 29209994; PMCID: PMC5778189.