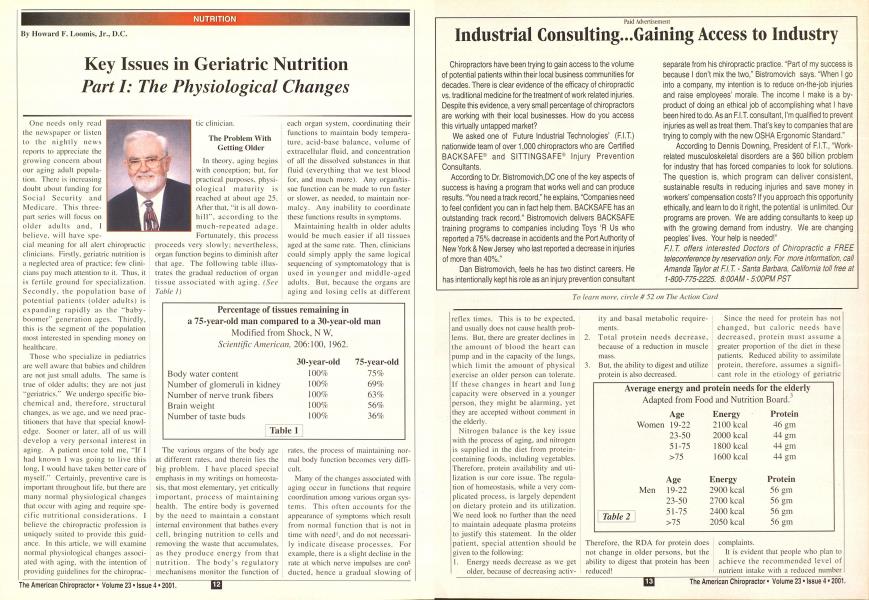
One needs only read the newspaper or listen to the nightly news reports to appreciate the growing concern about our aging adult population. There is increasing doubt about funding for Social Security and Medicare. This three-part series will locus on older adults and, I believe, will have spe- cial meaning lor all alert chiropractic clinicians. Firstly, geriatric nutrition is a neglected area of practice: lew clinicians pay much attention to it. Thus, it is fertile ground for specialization. Secondly, the population hase of potential patients (older adults) is expanding rapidly as the ""baby-boomer" generation ages. Thirdly. this is the segment of the population most interested in spending money on healthcare. Those who specialize in pediatrics are well aware that babies and children are not just small adults. The same is true of older adults: they are not just ""geriatrics." We undergo specific biochemical and. therefore, structural changes, as we age. and we need practitioners that have that special knowledge. Sooner or later, all of us will develop a very personal interest in aging. A patient once told me, '"If I had known I was going to live this long, I would have taken better care of myself." Certainly, preventive care is important throughout life, but there are many normal physiological changes that occur with aging and require specific nutritional considerations. I believe the chiropractic profession is uniquely suited to provide this guidance. In this article, we will examine normal physiological changes associated with aging, with the intention of providing guidelines for the chiroprac- tic clinician. The Problem With Getting Older In theory, aging begins with conception: but. for practical purposes, physiological maturity is reached at about age 25. After that, "it is all down-hill". according to the much-repeated adage. Fortunately, this process proceeds very slowly: nevertheless, organ function begins to diminish after that age. The following table illustrates the gradual reduction of organ tissue associated with aging. (Sec Table I) The various organs of the body age at different rates, and therein lies the big problem. I have placed special emphasis in my writings on homeosta-sis. that most elementary, yet critically important, process of maintaining health. The entire body is governed by the need to maintain a constant internal environment that bathes every cell, bringing nutrition to cells and removing the waste that accumulates. as they produce energy from that nutrition. The body's regulatory mechanisms monitor the function of each organ system, coordinating their functions to maintain body temperature, acid-base balance, volume of extracellular fluid, and concentration of all the dissolved substances in that fluid (everything that we test blood for. and much more). Any organ/tissue function can be made to run faster or slower, as needed, to maintain normalcy. Any inability to coordinate these functions results in symptoms. Maintaining health in older adults would be much easier if all tissues aged at the same rate. Then, clinicians could simply apply the same logical sequencing of symptomatology that is used in younger and middle-aged adults. But, because the organs are aging and losing cells at different rates, the process of maintaining normal body function becomes very difficult. Many of the changes associated with aging occur in functions that require coordination among various organ systems. This often accounts for the appearance of symptoms which result from normal function that is not in time with need1, and do not necessarily indicate disease processes. For example, there is a slight decline in the rate at which nerve impulses are conducted, hence a gradual slowing of Percentage of tissues remaining in a 75-year-old man compared to a 30-year-oid man Modified from Shock. N W, Scientific American, 206:100. 1962. Body water content Number of glomeruli in kidney Number of nerve trunk fibers Brain weight Number of taste buds 30-year-old 75-year-old 100% 75% 100% 69% 100% 63% 100% 56% 100% 36% Table 1 reflex times. This is to be expected, and usually does not cause health problems. But, there are greater declines in the amount of blood the heart can pump and in the capacity of the lungs, which limit the amount of physical exercise an older person can tolerate. If these changes in heart and lung capacity were observed in a younger person, they might be alarming, yet they are accepted without comment in the elderly. Nitrogen balance is the key issue with the process of aging, and nitrogen is supplied in the diet from protein-containing foods, including vegetables. Therefore, protein availability and utilization is our core issue. The regulation of homeostasis, while a very complicated process, is largely dependent on dietary protein and its utilization. We need look no further than the need to maintain adequate plasma proteins to justify this statement. In the older patient, special attention should be given to the following: 1. Energy needs decrease as we get older, because of decreasing activ- ity and basal metabolic requirements. Total protein needs decrease, because of a reduction in muscle mass. But, the ability to digest and utilize protein is also decreased. Therefore, the RDA for protein does not change in older persons, but the ability to digest that protein has been reduced! Since the need for protein has not changed, but caloric needs have decreased, protein must assume a greater proportion of the diet in these patients. Reduced ability to assimilate protein, therefore, assumes a significant role in the etiology of geriatric complaints. It is evident that people who plan to achieve the recommended level of nutrient intake with a reduced number Average energy and protein needs for the elderly Adapted from Food and Nutrition Board.' Table 2 Age Energy Protein Women 19-22 2100 kcal 46 gm 23-50 2000 kcal 44 gm 51-75 1800 kcal 44 gm >75 1600 kcal 44 gm Age Energy Protein Men 19-22 2900 kcal 56 gm 23-50 2700 kcal 56 gm 51-75 2400 kcal 56 gm >75 2050 kcal 56 am of calories will need to select foods of high nutrient density. Choices such as alcohol and high-caloric foods must be replaced with high-density foods and supplemental food enzymes to enhance : absorption and utilization. It is my belief that chiropractors see many recurring subluxation patterns in ; elderly patients that result from vis- cero-somatic reflexes. These occur when dietary changes have not been made to compensate for diminished j organ function and secretion, such as ! reduction in protein and fat intake. | Let's examine specific changes in i physiology that occur with aging. Salivary Glands Saliva secretion decreases with degeneration in the size of the salivary glands by age 60.2 This reduces the amount of saliva available to lubricate food. Swallowing may become more difficult. It may lead to the use of softer and creamer foods high in fat and starch, possibly as a way to compensate for the lack of natural lubricants in the saliva. These foods only add calories. Diminished salivary secretion also reduces the amount of amylase secreted from the parotid glands, and has an effect on the amount of starch that is predigested in the stomach. There is also a lipase secreted from the sublin-gual glands, and a protease secreted from the submandibular glands.4 These salivary enzymes do not have time to accomplish much digestion in j the mouth, but fortunately continue to | work in the esophagus and cardiac por- j tion of the stomach until the pH of that j compartment is reduced below 3.0. j This takes 30 to 60 minutes in a young [ adult.5 Hospital studies have proven it | requires much longer in the elderly, if it can be accomplished at all. Hydrochloric Acid Secretion A decline in hydrochloric acid secre- j tion is almost universal, with one-third ! of all people over 60 failing to secrete I any at all.6 This decline has adverse 1 effects on the absorption of calcium, I vitamin B1-. iron, and on the utilization j of protein. j Hydrochloric acid serves two pur- ! poses in the stomach. The first is to | react with pepsinogen. convening it to ' pepsin, and activating its proteolytic ;. capabilities. The second is to maintain | the pH of the stomach below 5.0. so that pepsin can act on protein, i Hydrochloric acid does not hydrolyze I (digest) protein, but reduced j hydrochloric acid secretion severely I compresses protein digestion. Obvi- i ously. supplementing HC1 will not I improve digestion.7 j Esophagus and Cardiac Portion j of the Stomach ! When food is masticated, it comes in j contact with moisture and amylase in j saliva. If the food consumed is raw. | the indigenous enzymes of the food | work with the salivary amylase to | begin digestion. Although swallowing j prevents food from remaining in the I mouth long enough for any significant j amount of digestion to occur, the i enzymes continue working as long as I they remain in a pH range of 3.0 to 9.0. I This occurs in the esophagus and car- | diac portion of the stomach, where the j resting pH is between 5.0 and 6.0. In j this "predigestive stomach'"8, a consid- | erable amount of digestive work can be j accomplished, if exogenous food j enzymes, either indigenous to the raw j food ingested or from a supplemental I source, are present. j More than seventy years ago. Olaf j Bergeim conducted a series of experiments on salivary digestion at the Laboratory of Physiological Chemistry in the University of Illinois College of Medicine, in Chicago. He found an average of 59% to 76% of ingested carbohydrates are rendered soluble within 15 to 30 minutes after a meal, and he concluded, if food is chewed properly. "... a very considerable degree of starch digestion may be brought about by saliva."* If salivary amylase, which does not work at a pH below 5.0. can digest 59% to 76% of ingested carbohydrates within 15 to 30 minutes, imagine how much carbohydrate, protein, and fat can be digested by exogenous plant enzymes, which go on working at pH levels as low as 3.0. In a study conducted in 1940 by J. M. Beazell. at the Northwestern University Medical School in Chicago, eleven clinically normal young adult males were led a test meal of known carbohydrate content, and then the food was withdrawn from the stomach after 30 minutes. In the recovered material. 39.8% of the carbohydrate content had been digested during that 30-minute period, prior to the secretion of HC1.1" Changes in Gastric Motility The motility (capability of movement) of the gastrointestinal tract is essential for mixing food with digestive enzymes and for the normal elimination of waste products. Decrease in gastric motility has a negative effect on digestion, because the food mass may not become thoroughly mixed with digestive secretions. There are, however, benefits that may result from an increase in absorption time, but these benefits can only be realized if adequate digestion has occurred. The inclusion of enzyme-containing foods in the diet or the use of supplemental food enzymes can achieve improved digestion. Fibromyalgia and Chronic Pain Syndromes This author believes decreased HC1 secretion and gastric motility may manifest themselves as recurring sub-luxations found in the middle thoracic spine (T5 to T9). when protein has not been digested by the geriatric patient. This mechanism can also account for many cases of so-called fibromyalgia and chronic pain syndrome.11 When digestion is incomplete, large polypep-tide and polysaccharide molecules can cross the gut wall.12 This triggers an immune response which has been referred to as a '"physiological leucocy-tosis."1-1 The result is the formation of circulating immune complexes which are the leading cause of fibromyalgia. They can retard healing, promote and prolong pain from inflammatory processes, and reduce immune defense competency." Pancreas The secretion of most digestive enzymes declines, but the extent ol each decrease, and the age at which it occurs has not been fully established. Depending on the extent of the decrease, food may be either incompletely digested, or require a longer time for complete digestion. It has Continued on Page 50 ..from Pciifc 14 , long been suspected that the pancreas i is not capable of elaborating all of the \ enzymatic secretion it has been given j credit for in the past. Now, research j has proven that, at least some, intact i digestive enzymes are absorbed by the j intestine, and are subsequently re- j secreted by the pancreas.14 This, at least, implies the possibility that enzymes contained in the diet, or sup plemental food enzymes can follow the ; same route alter performing digestive ! activity in the stomach. j Mnlubsorption i Absorption of many nutrients is ! reduced when there is degeneration of j the intestinal lining. Paramount, in my j opinion, is the decreased secretion of | disaccharidases. from the brush border | of the jejunum, with increased suscep- | tibility to poor digestion of white sugar I (sucrose), grains (maltose), and dairy j products (lactose). This degeneration j occurs in folacin deficiency, when new | cells of the intestinal wall fail to regen- ! erate as fast as old cells are destroyed, i Chronic diseases also result in j impaired absorption. Protein deficiency, which can result in a decrease in I the synthesis of carrier proteins needed I for absorption, reduces the uptake of j nutrients such as iron and calcium. | Colon | A major problem arises when j decreased motility of the lower gas- | irninlcsiinal tract causes constipation j and. in some cases, leads to an increase ! in infections. The longer food remains | in contact with the intestinal wall, the j greater the possibility of adverse j effects from toxic and/or carcinogenic j substances. This protein putrefaction, j and the resulting autointoxication j (indican) has been well-documented.IS Maintaining a diet that provides 30 to 40 grains of dietary fiber will help reduce these effects. Changes in Kidney Function As a person ages, the rate of blood flowing through the kidneys is decreased to 50% of the normal adult capacity. This means that less blood reaches the kidney filtering system, through which the waste products of metabolism are eliminated, and the nutrients are returned to general circu- lation. In addition, older people have a : reduced capacity to form either a more concentrated or more dilute urine. As a result, there is a decline in their abili- ! ty to handle large amounts of waste | products (particularly urea and sodi- | urn) or water. I Kidney function influences the com- ] position of the fluid surrounding indi- i vidual cells, which is normally maintained within very narrow limits. The i speed with which older people are able I to cope with changes in blood and j intracellular fluid composition after consuming excess acid-forming or base-forming substances may be as little as one-fourth the speed of younger people. This is merely one example of changes in the rate at which the body can adjust to stress. Alterations in the Blood Vessels Alterations in the blood vessels— such as the narrowing of the lumen, thickening of the wall, and replacement of elastic muscle fibers with non-elastic material—reduce their capacity to effectively carry nutrients to body cells. Among other things, this reduces secretions of hormones. Hormones regulate a wide range of physiological processes that have direct, and indirect effects on the nutrition of the cells and. therefore, on the whole body. By controlling the diameter of blood vessels, the endocrine glands regulate the amount of blood and. therefore, the nutrients that reach the tissues. In aging people, there is a greater restriction in the size of the blood vessels leading to the kidneys than in the size of those leading to the brain (an example of ensuring a more adequate blood supply to the more vital centers). However, this dramatically reduces the ability of the body to deliver waste products to the kidneys and lungs for removal. This compounds the possibility of fibromyalgia and chronic pain syndromes, as well as viscero-somatic reflex activity in the geriatric patient. SUMMARY Reduced caloric and protein needs of the elderly must be offset by an increase in their digestive abilities and improved nutrient density of their diets. As chiropractors, we are uniquely qualified to determine, by case his- lory, examination, and urinalysis, early deviations from homeostasis. This is particularly important in the geriatric patient, since the ability to digest and assimilate protein is naturally compromised. Taking care of the older patient can be very rewarding, as aging gracefully is something we all desire. Howard F. Looniis. Jr., DC. president of Enzyme Formulations, Inc., has an extensive background in enzymes and enzyme formulations. As president of 21st Century Nutrition, Inc., for fifteen years, he has forged a remarkable career as an educator, having conducted over 400 seminars to date, in the United States, Canada, Germany, and Australia, on the diagnosis and treatment of enzyme deficiency syndromes. Call 21s' Century Nutrition at 1-800-662-2630 for more information. REFERENCES /. Anything Can Cause Anylhini;. VV D Harper. DC. published privately. 1964. 2. Nutrition and Diet Therapy. S R Williams. PhD. Times Mirror/Moshy College Publishing. 1985. .1. Food and Nutrition Hoanl. National Research Council, Recommended dietary allowances. 9lh ed.. New York: National Academy Press. 1980. Textlwok of Medical I'liysiology. A C Guy- ton. Ml). W B Saunders Co.. 7th ed.. 1986. "Improve Digestion with Plant Enzymes". H F Loomis, DC. The American Chirttpractor. February 1990. Introductory Nutrition. H A Outline. PhD. Times Mirror/Moshy College Publishing. 1986. "Indigestion", by H F Loomis. DC. The American Chiropractor. April 1988. Enzyme Nutrition. F Howell. MD. Avery Publishing Group. Wayne. NJ. 1985. "Salivary Digestion in the Human Stomach and Intestines". 0 Bergeim. Archives of Internal Medicine. 1926: 37:1 12. "A Re-examination of the Role of the Stom ach in the Digestion of Carbohydrates and Protein". J M Beazell. American Journid of Pliyxiolofiy. 1941: 132:42.50. "Fihromyalgia. Chronic Pain and the Leaky Gut Syndrome". Lanfranchi. Donovan. Deusler and Jaffe. Today's Chiropractic. October 1994. Intestinal Absorption of I'eptides. M I- Gard ner. School of Biomedical Sciences. Univer sity of Bradford-England. Academic Press. 1988. Cellular Pathology. Rudolph Virchow. pub lished in London. I860. "I:nteropancreatic Circulation of Digestive Enzymes". C Liehow. & S S Rolhman. American Journal of Physiology. 1974; 226:1077. "Evidence for Intestinal Toxemia, an Inescapable Clinical Phenomenon", by A Immerman. Journal of American Chiroprac tic Association. April I97K.D