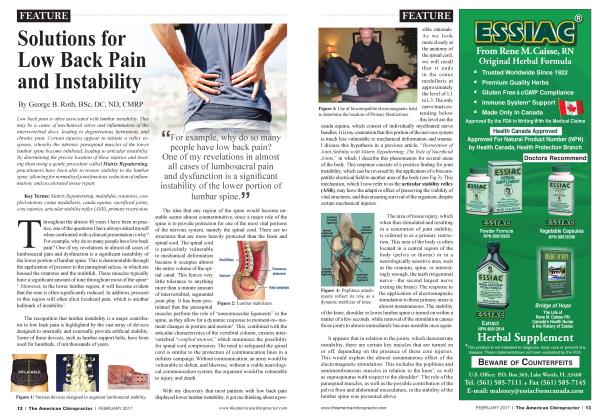
Presented, by invitation, at the 2nd Annual Conference of Canadian Chiropractic Research Centers Introduction "Frozen shoulder", according to many authors is a clinical disorder rather than a diagnosis. It is considered to be the final stage of a number of disorders which affect the shoulder.2 Synonyms include adhesive capsulitis,1-1-4 periarthritis,2-3 pericap-sulitis,-*--1 scapulocostal syndrome7 and degenerative tendinitis of the rotator cuff.2-' It affects females more often than males and is predominantly seen in the 40-70 year age range. It is unilateral in 909c of cases---"1-'' and usually follows a course of clinical development which involves 1) pain. 2) stiffening. 3) thawing. This course may last from 6 months to several years.5-9 No definitive diagnosis is available, however capsular fibrosis, thickening and contraction of the synovial membrane and protective periarticular muscle spasm are the hallmarks of the condition at the tissue level.2-7 Tensegrity Therapy®, is a new approach to the understanding of the mechanism of injury, and the manner in which the human body responds to these forces. It is based on a new model of the underlying structure of organic tissue—the Tensegrity Structural Made!—which appears to explain the complex interrelationship of all the structural components of the body. It extends the basic concept of the primacy of restriction, beyond the level of joint, muscle and ligament, to include all of the tissues of the body, as potential sources of dysfunction. The Tensegrity Structural Model holds that the body tissues are composed of interconnected tension icosolwdru (com- plex triangular trusses), j which inherently provide \ a balance between stabili-1 ty and mobility.5-6 This j structural model explains j many of the observed] phenomena related to | body support, movement, j response to stress and | trauma, as well as the effects of various thera-peutic interventions. This | theory has been venried j by several studies in recent years. According to Ingber, a key investigator who has proven the existence of this structural model: • "The principles of tensegrity apply at essentially every detectable size scale in the human body. At the macroscopic level, the 206 bones that constitute our skeleton are pulled up against the force of gravity and stabilized in a vertical form by the pull of tensile muscles, tendons and ligaments. In other words, in the complex tensegrity structure inside every one of us. bones are the compression struts, and muscles, tendons and ligaments [and all, interconnected fas-cial structures] are the tension-bearing members. "s This structural model explains the j physiologic changes, which manifest in injured or strained tissue. The apparent I'ibrosis of muscle and fascia can be seen as an altered electromechanical relationship at the molecular level. The tensegrity structure is, thus, converted from a neutral, flexible form to a strained, high-energy, linearly-stiffened mode as shown in Figure 1\ The principle of treatment is the release of fascial restrictions within the tensegrity structure—at the molecular level. It is theorized that compression of tissues results in a piezo-electric effect. This causes the electrons, which are associated with the chemical bonds in the involved tissues, to generate a form of intrinsic current. This effect has been demonstrated in bone repair, when it is placed under compression. A gentle, gradual pressure, referred to as induction, or a sudden movement, referred to as directional recoil, may be utilized. The traditional chiropractic adjustment may also accomplish this change, when applied to the appropriate site of involvement. Careful consideration is given to ail of the tissues of the body, since fascial structure is inherently interconnected.8 It should be noted that post-traumatic studies of pigs, found that internal organs (heart, kidneys, liver and spleen) were almost always injured in simulated motor vehicle accidents. These structures are fluid-filled and are, therefore, very dense, in relation to other tissues of the body. In the event of a traumatic blow to the body, these structures and their intervening fascia will absorb most of the force of impact. The potential for iniiaosseous lesions is also recognized as an important factor in many dysfunctional patterns. It has been the experience of the author that these tissues are often the sites of primary lesions, in otherwise resistant cases.* Tensegrity theory views frozen shoulder as one possible manifestation of an aberrant mechanical adaptation to primary foci of restriction. The determination of these primary foci and their resolution, are the goals of the practitioner, rather than simply addressing the site of symptoms. Patterns of tension created by the primary lesions and biomechanical compensations, such as shoulder restriction, are restored to normal. Methodology Case files were chosen on the basis of restriction of abduction of the shoulder to less than 90°. As this was a retrospective study, the number of treatments were not uniform, however they averaged at 6 treatments with a range of 2-to-10 treatments in this group. Some contained measurements for internal and external rotation. The latter were performed at the limit of the passive range of the shoulder, or at 90°, whichever was less. The assessment was visual and/or goniometric. The data for this group was then analyzed for the rate and degree of resolution of restriction of motion and tabulated accordingly. Results (See Table Below) The mean improvement in abduction was 58.3°. For those cases in which internal and external rotation ranges were noted (3), the average improvement was 25° for internal rotation and 30° for external rotation. All but one of the individuals reported a significant reduction of pain and an improved active range of motion, as well as the ability to carry on the activities of daily living. Discussion Tensegrity Therapy®, is administered entirely on the basis of tissue compliance, as determined by the established protocols elaborated by the author. The primary foci of involvement, in the above cases, often involved the fascial structures within the torso, namely the investing fascia of the dense, water-filled viscera (heart, liver, kidneys and spleen). Other areas included the pelvis and long bones of the lower quadrant, as well as the spine and local structures within the upper limb, including the shoulder girdle. In general, treatment involves an application of gentle force to the restriction barrier with the aim of normalizing the intramolecular dynamics of the tensegrity structure. In most cases, any one lesion is resolved with one treatment. Several layers may need to be treated for clinical resolution. The presence of adhesive pathology, in the form of surgical scars and post-inflammatory adhesions, often requires adjunctive therapy in order to address these tissues. Conclusions Tensegrity Therapy®, represents a significant departure from the established protocols for the treatment of musculoskeletal disorders. It incorporates the newly confirmed structural characteristics of tissue to assess and treat primary foci of involvement. This process frees the practitioner from the tyranny of symptoms and focuses attention on the source of tissue dysfunction, which is seen as a manifestation of molecular forces rather than simply local tissue properties. Many practitioners who have incorporated this form of treatment into their practices have found similarly profound results in a wide range of conditions. It is recommended that further research be developed to determine the effectiveness of these approaches. It is the opinion of the author that Tensegrity Therapy®, represents a new horizon in our understanding of structural patho-physiology and our ability to address many resistant conditions, in a more deliberate, scientific and successful manner. Dr. George Roth is the developer of Tensegrity Therapy® and teaches seminars which are co-sponsored by Logan College of Chiropractic. For more information contact Wellness Systems, Inc., at:905-880-0101; Toll-free: 1-877-905-ROTH; Fax: 905-880-0650; or email: Roth@ WellnessSys-tems.com. You can also visit his web site at: www. WellnessSystems. com. References: Anncxton M: Anhrography can help free "t'rewen shoulder." JAMA 241:875-876. 1979. Baleman JH: The Slumltlcr and Neck, W.B. Saun- ders. Philadelphia. 1972. Caillct R: Soft Tissue Pain anil Disability. FA. Davis. Philadelphia. 1977. Caillcl R: Shoulder Pain. F.A. Davis. Philadel phia. 1%6. Ingher DK: The Archileclure <il" Lite. Sci Am 48- 57, January. 1998. Levin SM: The Importance of Soft Tissues for Structural Support of the Body: in D'Ambrogio KJ. Roth GB: Positional Release Therapy: Assessment iv Treatment of Musctlloskelelal Dys function. Moshy-Harcourt. St. Louis. 1997. Neviaser JS: Adhesive capsulilis of shoulder: study of pathological findings in periarthritis of shoulder. J Bone Joint Surf; 27:211-222. 1945. Roth GB: Tensearily Therapy®: Study Guide. Wellness Systems. Tottenham. ON, 1999. Thompson WAL. Kopell HP: The components of the fro/en shoulder. Bull /Vf Acud Med J6:5()l- 509. 196(1. O Duration of Number of Initial Final Patient Age Sex Condition Treatments Abduction Range (°) Abduction Range («) Case 1 47 F 18 months 4 60 135 Case 2 61 F 6 years 8 90 135 Case 3 69 M 4 years 6 80 135 Case 4 42 F 8 months 2 70 135 Case 5 72 M 10 years 4 90 120 Case 6 53 F 12 months 4 70 150