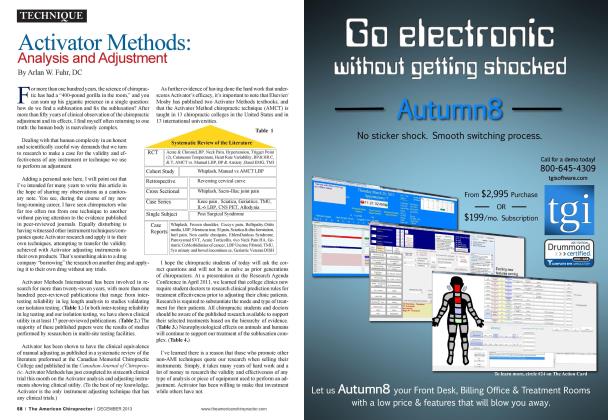
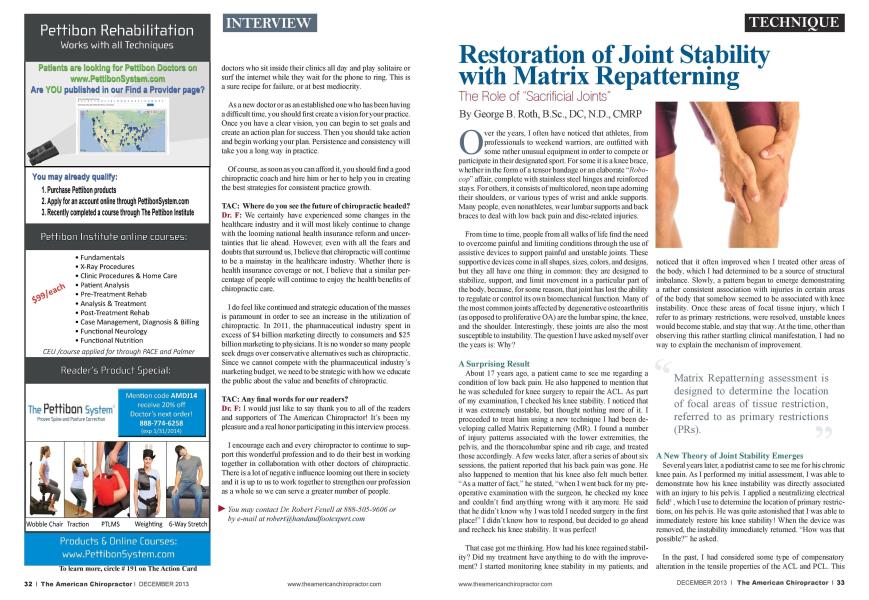
O ver the years. I often have noticed that athletes, from professionals to weekend warriors, are outfitted with some rather unusual equipment in order to compete or participate in their designated sport. For some it is a knee brace, whether in the form of a tensorbandage oran elaborate "Robo-cop" affair, complete with stainless steel hinges and reinforced stays. For others, it consists of multicolored, neon tape adorning their shoulders, or various types of wrist and ankle supports. Main people, even nonathlctcs. w car lumbar supports and back braces to deal with low back pain and disc-related injuries. From time to time, people from all walks of life find the need to overcome painful and limiting conditions through the use of assistivc devices to support painful and unstable joints. These supportive devices come in all shapes, sizes, colors, and designs, but they all have one thing in common: they arc designed to stabilize, support, and limit movement in a particular part of the body, because, for some reason, that joint has lost the ability to regulate or control its own bioniechanical function. Mam of the most common joints affected by degenerative ostcoarthritis (as opposed to proliferate c OA) are the lumbar spine, the knee, and the shoulder. Interestingly, these joints arc also the most susceptible to instability. The question I have asked myself over the years is: Why? A Surprising Result About 17 years ago. a patient came to see me regarding a condition of low back pain. He also happened to mention that he was scheduled for knee surgery to repair the ACL. As part of my examination. I checked his knee stability. I noticed that it was extremely unstable, but thought nothing more of it. I proceeded to treat him using a new technique I had been developing called Matrix Rcpattcrning (MR). I found a number of injury patterns associated with the lower extremities, the pelvis, and the thoracolumbar spine and rib cage, and treated those accordingly. A few weeks later, after a scries of about six sessions, the patient reported that his back pain was gone. He also happened to mention that his knee also felt much better. "As a matter of fact." he stated, "w hen I went back for my pre-opcrativc examination with the surgeon, he checked my knee and couldn't find anything wrong with it anymore. He said that he didn't know why I was told I needed surgery in the first place!" I didn't know how to respond, but decided to go ahead and rcchcck his knee stability. It was perfect! That case got me thinking. How had his knee regained stability? Did my treatment have anything to do with the improvement? I started monitoring knee stability in my patients, and noticed that it often improved when I treated other areas of the bod\'. which I had determined to be a source of structural imbalance. Slowly, a pattern began to emerge demonstrating a rather consistent association with injuries in certain areas of the body that somehow seemed to be associated with knee instability. Once these areas of focal tissue injury, which I refer to as primary restrictions, were resolved, unstable knees would become stable, and stay that way. At the time, other than obscn ing this rather startling clinical manifestation. I ted no way to explain the mechanism of improvement. A New Theory of Joint Stability Emerges Several years later, a podiatrist came to sec me for his chronic knee pain. As I performed my initial assessment. I was able to demonstrate how his knee instability was directly associated with an injury to his pelvis. I applied a neutralizing electrical field1. which I use to determine the location of primary restrictions, on his pelvis. He was quite astonished that I was able to immediately restore his knee stability! When the device was removed, the instability immediately returned. "How was that possible?" he asked. In the past. I had considered some type of compensatory alteration in the tensile properties of the ACL and PCL. This was an immediate change, though, and I could never understand how ligaments that had been lax could suddenly increase in tone. In addition, my patient was a fellow health professional, someone highly respected in the field of podiatric medicine who worked closely with a number of orthopedic surgeons. I needed to consider my explanation carefully. So. I considered the evidence: The knee was initially profoundly unstable. I temporarily neutralized the primary restriction in his pelvis using a local electromagnetic field. The knee instantly stabilized. I removed the device. The knee once again became unstable, and instantly. I thought: Wliat works that fast in the body? Could it be a ncuromuscular response? What muscle could possibly affect stability of the knee? How was this being mediated? Recent studies have postulated the popliteus as an important dynamic stabilizer of the knee1-2. It is intricately attached to several internal structures of the knee, including the lateral meniscus, the posterior capsule of the knee, the PCL. and the MCL\ I decided to look into the possible role this muscle played with the function of the knee. I also decided to investigate the possible role of appropriately targeted treatment, such as Matrix Repattcrning. which might help restore stability to the knee, and thus promote healing of this joint. The typical clinical approach to an unstable knee is through exercise of the large muscle groups, or if all else fails, surgery for the so-called "torn ACL or PCL." The purported incidence of actual tears of these ligaments appears to be much less than indicated by radiological reports. Surgical reports often contradict the reported findings of radiologists in these cases4. Recently. I also have discovered that anterior instability of the knee often is accompanied by reduced tone of the biceps femo-ris. and that treatment of the pelvis often restores tone in this muscle as well as knee stability, as measured with an anterior drawer test. Additional muscular and fascial associations appear to mediate ankle stability. In the shoulder, a similar mechanism was identified regarding the possible role of the supraspinatus as a stabilizer of the glcno-humeral joint5. Joint Stability as a Symptom of Core Injury Matrix Rcpatterning assessment is designed to determine the location of focal areas of tissue restriction, referred to as primary restrictions (PRs). PRs arc often located in areas of the body remote from the area of symptoms, which may be compensatory to the effects of the PRs. As I reviewed the areas containing the primary restrictions that seemed to be associated with instability. I noticed that they were invariably located in the torso and pelvis—the so-called core structures of the body. Treatment of these areas usually resulted in restoration of stability in the involved joints, which appeared to occur primarily in peripheral joints. The one exception was the lumbar spine, which is located in the core region. However, this exception proved to be a key to my understanding of this important mechanism. I postulated that the purpose of instability was to protect the core structures from additional mechanical strain and potential debilitating or even life-threatening damage. In particular. I reasoned that one of the primary goals of this protective mechanism might be to protect a particularly vital structure, namely the spine and more importantly, the spinal cord. The knee, ankle, shoulder, and wrist joints, which arc completely dependent on soft-tissue for stabilization, could be considered "sacrificial gears." This is a term used with industrial machinery, such as printing presses, where specific gears constructed of less robust materials arc situated at non-critical points in the device. These arc deliberately designed to fail and disintegrate should the machinery become severely jammed, thus protecting more critical components. Could the unstable joints in fact be sacrificial joints? (see Figure 1) But what about the lower lumbar spine? The spinal cord is a key. core structure that must be protected, but. as we know, the spinal cord ends at the level of L2 or L3. Thus, the neurological structures of the lower lumbar spine, composed of separate nerve tracts each protected by the meninges (cauda cquina). arc much less vulnerable to serious damage. People with lower lumbar injun tend to have much less debilitating impairment than those with direct spinal cord injuries. Thus, the response of the lower lumbar spine fits the model of instability that I had been formulating. An Emerging Paradigm in Structural Therapy— Turning Joint Stability Back On Matrix Rcpattcrning is a gentle form of manual therapy based on a recent understanding of the infrastructure of the body, specifically the intraccllular and extracellular matrix, and their influence on structural, mechanical, and physiological properties of the body. The basic premise is that specific manual therapy applied to areas of the body identified as primary restrictions can help restore the functional capacity of tissue, restoring its clastic and electrochemical properties'' "x. Primary restrictions arc often located in the deep core stnictures within the skeletal frame (referred to as intraosseous lesions) and the fluid-filled thoracic and abdominopclvic areas, directly related to the spine, pelvis, and rib cage. These injun patterns are often associated with impact injuries, such as falls, sports injuries, and motor vehicle collisions. Other forms of treatment, such as traditional chiropractic care including SMT. may also be effective at resolving some of these issues. Remarkably, treatment of primary restrictions often located in remote parts of the body appears to immediately restore stability in the affected joints. What could account for this response? My current theory is that there may be a feedback mechanism mediated by spinal reflexes or mechanical electrochemical signals generated within the extracellular matrix (ECM)1'. These systems may be able to monitor potentially threatening injuries, and respond by triggering inhibitory or excitatory efferent neurons (spinal/ neurological level), or via the production of electrochemical signals to activate specific tonal structural proteins within the ECM. Whatever the mechanism may be. it appears to allow the body to rapidly modulate stability of the peripheral, ap-pcndicular joints. Practitioners trained in Matrix Rcpat-tcrning have confirmed that joint stability" often is restored when the underlying primary restrictions arc properly addressed. In this way. they have been able to help mam conditions associated with joint instability, resulting in significant clinical improvement. Further research is also required to assess the effectiveness of this approach on the possible reversal or prevention of degenerative changes associated with these joints. References: Anatomy and Function of the Poplitcus Muscle. I Maclnlyrc. E-book. 2009. Electromyographic Study of the Poplitcus Muscle in the Dynamic Stabilization of the Poslcrolalcral Comer Structures of (he Knee, K Schinhan. et al. Am J Sports Med. Vol. 39. No. 1. 173-179. January. 2011. The role of the poplitcofibular ligament and the tendon of poplitcus in providing stability in the human knee. Pasquc. C. ct al. University of Cincinnati. J Bone Joint Surg Br. 85 (2): 292-298. March 2003. Imaging the Knee: Ligaments. DB Niss- man el al.. Applied Radiology. Vol. 37. No. 12. Dec. 2008. Function of the Supraspinatus Muscle and its Relation to the Supraspinatus syndrome - An experimental in Man. B Van Linge. JD Mulder. Journal of Bone and Joint Surgery. Vol. 45B, No. 4. November 1963. pp 750-754. The Architecture of Life. DE Ingbcr. Scien tific American. Vol. 1. January 1998. Streaming and piezoelectric potentials in connective tissues. LAMacGuinlic. In: Blank M (ed.) Electromagnetic fields: biological interactions and mechanisms. Advances in Chemistry Scries 250. American Chemical So ciety. Washington DC. ch. 8. pp 125-142. 1995. The Matrix Rcpattcrning Program for Pain Relief. GB Roth. New Harbinger Publications. Oakland. CA. 2005. 9. The Extracellular Matrix and Ground Regulation. Basis for a Holistic Biological Medicine. A Pischinger. North Atlantic Books. Bcrklev. 2007. Dr. George Roth has been in practice since 1978, and is recognized worldwide as an authority in the treat- menl of niusciiloskeletal and structural disorders. He is the co-author of Positional Release Therapy: Assessment and Treatment of.\ lusailoskeletal Dysfunction (Elsevier Science), and the author of The Matrix Repatterning Program for Pain Relief (Sew Harbinger Publications). He currently practices in Newmarket Ontario.