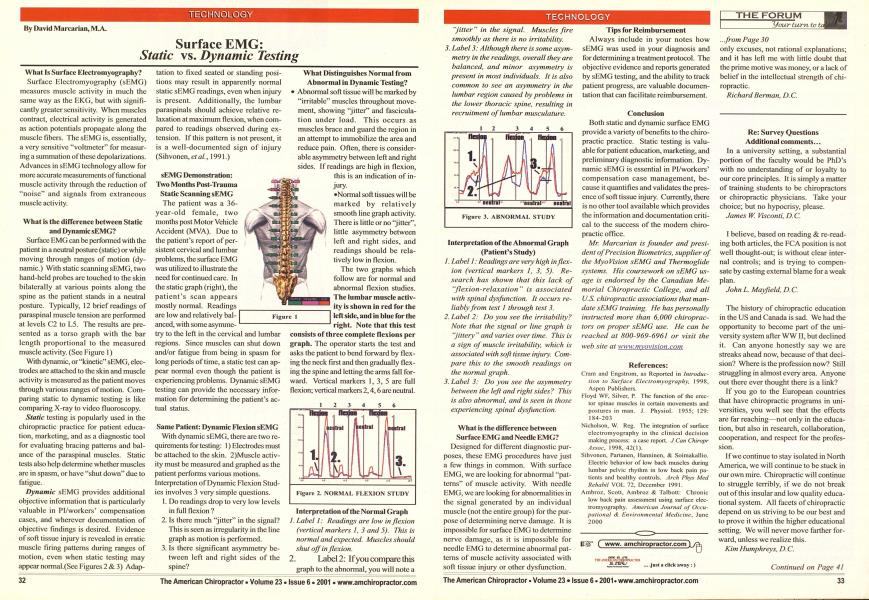
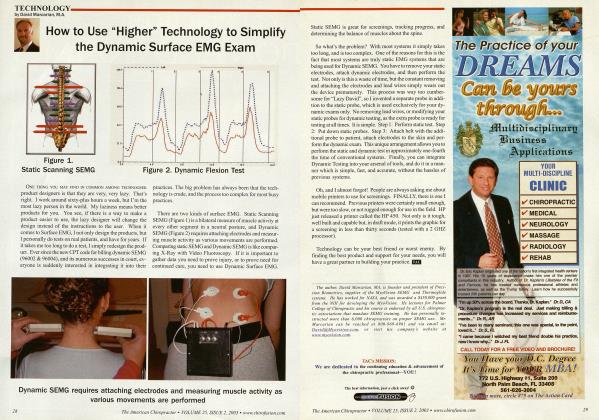
What Is Surface Electromyography? Surface Electromyography (sEMG) measures muscle activity in much the same way as the EKG, but with significantly greater sensitivity. When muscles contract, electrical activity is generated as action potentials propagate along the muscle fibers. The sEMG is, essentially, a very sensitive "voltmeter" for measuring a summation of these depolarizations. Advances in sBMG technology allow for more accurate measurements of functional muscle activity through the reduction of "noise" and signals from extraneous muscle activity. What is the difference between Static and Dynamic sEIMG? Surface EMG can be performed with the patient in a neutral posture (static) or while moving through ranges of motion (dynamic.) With static scanning sEMG, two hand-held probes are touched to the skin bilaterally at various points along the spine as the patient stands in a neutral posture. Typically, 12 brief readings of paraspinal muscle tension arc performed at levels C2 to L5. The results are presented as a torso graph with the bar length proportional to the measured muscle activity. (See Figure 1) With dynamic, or "kinetic" sEMG, electrodes are attached to the skin and muscle activity is measured as the patient moves through various ranges of motion. Comparing static to dynamic testing is like comparing X-ray to video fluoroscopy. Static testing is popularly used in the chiropractic practice for patient education, marketing, and as a diagnostic tool for evaluating bracing patterns and balance of the paraspinal muscles. Static tests also help determine whether muscles are in spasm, or have "shut down" due to fatigue. Dynamic sEMG provides additional objective information that is particularly valuable in Pl/workers' compensation cases, and wherever documentation of objective findings is desired. Evidence of soft tissue injury is revealed in erratic muscle firing patterns during ranges of motion, even when static testing may appear norma!.(Scc Figures 2 & 3) Adap- tation to fixed seated or standing positions may result in apparently normal static sEMG readings, even when injury is present. Additionally, the lumbar paraspinals should achieve relative relaxation at maximum flexion, when compared to readings observed during extension. If this pattern is not present, it is a well-documented sign of injury (Sihvonen,e/a/., 1991.) sEMG Demonstration: Two Months Post-Trauma Static Scanning sEMG The patient was a 36-year-old female, two months post Motor Vehicle Accident (MVA). Due to the patient's report of persistent cervical and lumbar problems, the surface EMG was utilized to illustrate the need for continued care. In the static graph (right), the patient's scan appears mostly normal. Readings are low and relatively balanced, with some asymme- try to the left in the cervical and lumbar regions. Since muscles can shut down and/or fatigue from being in spasm for long periods of time, a static test can appear normal even though the patient is experiencing problems. Dynamic sEMG testing can provide the necessary information for determining the patient's actual status. Same Patient: Dynamic Flexion sEMG With dynamic sEMG, there arc two requirements for testing: 1) Electrodes must be attached to the skin. 2)Muscle activity must be measured and graphed as the patient performs various motions. Interpretation of Dynamic Flexion Studies involves 3 very simple questions. 1. Do readings drop to very low levels in full flexion ? 2 Is there much "jitter" in the signal? This is seen as irregularity in the line graph as motion is performed. 3. Is there significant asymmetry between left and right sides of the spine? What Distinguishes Normal from Abnormal in Dynamic Testing? Abnormal soft tissue will be marked by "irritable" muscles throughout movement, showing "jitter" and fascicula-tion under load. This occurs as muscles brace and guard the region in an attempt to immobilize the area and reduce pain. Often, there is considerable asymmetry between left and right sides. If readings are high in flexion, this is an indication of injury. •Normal soft tissues will be marked by relatively smooth line graph activity. There is little or no "jitter", little asymmetry between left and right sides, and readings should be relatively low in flexion. The two graphs which follow are for normal and abnormal flexion studies. The lumbar muscle activity is shown in red for the left side, and in blue for the right. Note that this test consists of three complete flexions per graph. The operator starts the test and asks the patient to bend forward by flexing the neck first and then gradually flexing the spine and letting the arms fall forward. Vertical markers 1, 3, 5 arc full flexion; vertical markers 2,4,6 are neutral. Interpretation of the Normal Graph /. Label 1: Readings are low inflexion (vertical markers I, 3 and 5). This is normal and expected. Muscles should shut off in flexion. 1. Label 2: If you compare this graph to the abnormal, you will note a "jitter" in the signal. Muscles fire smoothly as there is no irritability. 3. Label 3: Although there is some asymmetry in the readings, overall they are balanced, and minor asymmetry is present in most individuals. It is also common to see an asymmetry in the lumbar region caused by problems in the lower thoracic spine, resulting in recruitment of lumbar musculature. Interpretation of the Abnormal Graph (Patient's Study) /. Label 1: Readings are very high inflexion (vertical markers 1, 3, 5). Research has shown that this lack of "flexion-relaxation " is associated with spinal dysfunction. It occurs reliably from test I through test 3. Label 2: Do you see the irritability? Note that the signal or line graph is "jittery " and varies over time. This is a sign of muscle irritability, which is associated with soft tissue injury. Com pare this to the smooth readings on the normal graph. Label 3: Do you see the asymmetry between the left and right sides? This is also abnormal, and is seen in those experiencing spinal dysfunction. What is the difference between Surface EMG and Needle EMG? Designed for different diagnostic purposes, these EMG procedures have just a few things in common. With surface EMG, we are looking for abnormal "patterns" of muscle activity. With needle EMG, we are looking for abnormalities in the signal generated by an individual muscle (not the entire group) for the purpose of determining nerve damage. It is impossible for surface EMG to determine nerve damage, as it is impossible for needle EMG to determine abnormal pat- • terns of muscle activity associated with soft tissue injury or other dysfunction. Tips for Reimbursement Always include in your notes how sEMG was used in your diagnosis and for determining a treatment protocol. The objective evidence and reports generated by sEMG testing, and the ability to track patient progress, are valuable documentation that can facilitate reimbursement. Conclusion Both static and dynamic surface EMG provide a variety of benefits to the chiropractic practice. Static testing is valuable for patient education, marketing, and preliminary diagnostic information. Dynamic sEMG is essential in Pi/workers' compensation case management, because it quantifies and validates the presence of soft tissue injury. Currently, there is no other tool available which provides the information and documentation critical to the success of the modern chiropractic office. Mr. Marcarian is founder and president of Precision Biometrics, supplier of the MyoVision sEMG and Thermoglide systems. His coursework on sEMG usage is endorsed by the Canadian Memorial Chiropractic College, and all U.S. chiropractic associations that mandate sEMG training. He has personally instructed more than 6,000 chiropractors on proper sEMG use. He can be reached at 800-969-6961 or visit the web site at www.myovision.com References: Cram and Engstrom, as Reported in Introduction to Surface Electromyography, 1998, Aspen Publishers. Kloyd WF, Silver, P. The Function of the erector spinae muscles in certain movements and postures in man. J. Physiol. 1955; 129: 184-203 Nicholson, W. Reg. The integration of surface elcctromyography in the clinical decision making process: a case report. J Can Chiropr A.ssoc, 1998, 42(1). Sihvonen, Partancn, Hanninen, & Soimakallio. Electric behavior of low back muscles during lumbar pelvic rhythm in low back pain patients and healthy controls. Arch Phys Med Rehahil VOL 72, December 1991. Ambroz, Scott, Ambroz & Talbott: Chronic low back pain assessment using surface elec-tromyography. American Journal of Occupational & Environmental Medicine, June 2000