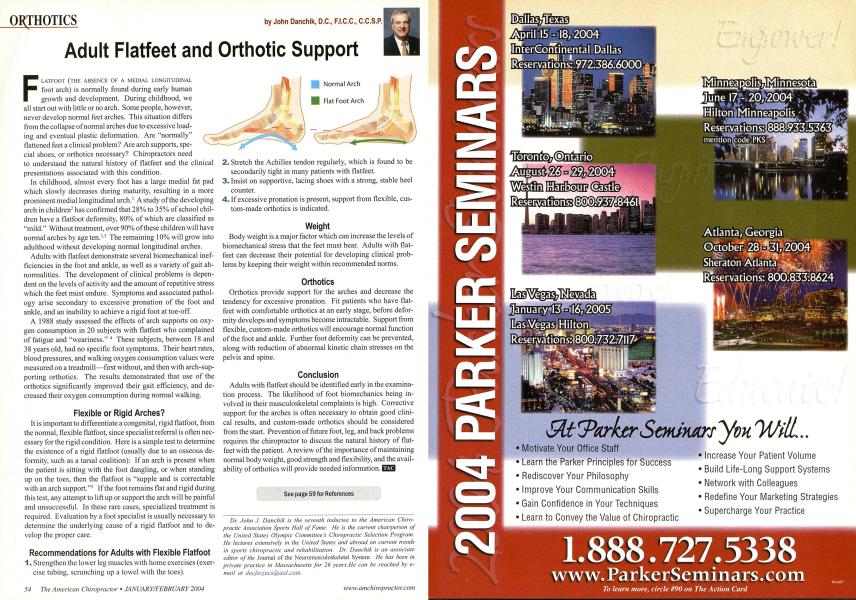
F LATFOOT (THE ABSENCE OF A MEDIAL LONGITUDINAL foot arch) is normally found during early human growth and development. During childhood, we all start out with little or no arch. Some people, however, never develop normal feet arches. This situation differs from the collapse of normal arches due to excessive loading and eventual plastic deformation. Are "normally" flattened feet a clinical problem? Are arch supports, special shoes, or orthotics necessary? Chiropractors need to understand the natural history of flatfeet and the clinical presentations associated with this condition. In childhood, almost every foot has a large medial fat pad which slowly decreases during maturity, resulting in a more prominent medial longitudinal arch.1 A study of the developing arch in children2 has confirmed that 28% to 35% of school children have a flatfoot deformity, 80% of which are classified as "mild." Without treatment, over 90% of these children will have normal arches by age ten.1-3 The remaining 10% will grow into adulthood without developing normal longitudinal arches. Adults with flatfeet demonstrate several biomechanical inefficiencies in the foot and ankle, as well as a variety of gait abnormalities. The development of clinical problems is dependent on the levels of activity and the amount of repetitive stress which the feet must endure. Symptoms and associated pathology arise secondary to excessive pronation of the foot and ankle, and an inability to achieve a rigid foot at toe-off. A 1988 study assessed the effects of arch supports on oxygen consumption in 20 subjects with flatfeet who complained of fatigue and "weariness." 4 These subjects, between 18 and 38 years old, had no specific foot symptoms. Their heart rates, blood pressures, and walking oxygen consumption values were measured on a treadmill—first without, and then with arch-supporting orthotics. The results demonstrated that use of the orthotics significantly improved their gait efficiency, and decreased their oxygen consumption during normal walking. Flexible or Rigid Arches? It is important to differentiate a congenital, rigid flatfoot, from the normal, flexible flatfoot, since specialist referral is often necessary for the rigid condition. Here is a simple test to determine the existence of a rigid flatfoot (usually due to an osseous deformity, such as a tarsal coalition): If an arch is present when the patient is sitting with the foot dangling, or when standing up on the toes, then the flatfoot is "supple and is correctable with an arch support."5 If the foot remains flat and rigid during this test, any attempt to lift up or support the arch will be painful and unsuccessful. In these rare cases, specialized treatment is required. Evaluation by a foot specialist is usually necessary to determine the underlying cause of a rigid flatfoot and to develop the proper care. Recommendations for Adults with Flexible Flatfoot 1. Strengthen the lower leg muscles with home exercises (exercise tubing, scrunching up a towel with the toes). Stretch the Achilles tendon regularly, which is found to be secondarily tight in many patients with flatfeet. Insist on supportive, lacing shoes with a strong, stable heel counter. If excessive pronation is present, support from flexible, cus tom-made orthotics is indicated. Weight Body weight is a major factor which can increase the levels of biomechanical stress that the feet must bear. Adults with flat-feet can decrease their potential for developing clinical problems by keeping their weight within recommended norms. Orthotics Orthotics provide support for the arches and decrease the tendency for excessive pronation. Fit patients who have flat-feet with comfortable orthotics at an early stage, before deformity develops and symptoms become intractable. Support from flexible, custom-made orthotics will encourage normal function of the foot and ankle. Further foot deformity can be prevented, along with reduction of abnormal kinetic chain stresses on the pelvis and spine. Conclusion Adults with flatfeet should be identified early in the examination process. The likelihood of foot biomechanics being involved in their musculoskeletal complaints is high. Corrective support for the arches is often necessary to obtain good clinical results, and custom-made orthotics should be considered from the start. Prevention of future foot, leg, and back problems requires the chiropractor to discuss the natural history of flat-feet with the patient. A review of the importance of maintaining normal body weight, good strength and flexibility, and the availability of orthotics will provide needed information. I See page 59 for References Dr. John J. Danchik is the seventh inductee to the American Chiropractic Association Sports Hall of Fame. He is the current chairperson of the United States Olympic Committee s Chiropractic Selection Program. He lectures extensively in the United Slates and abroad on current trends in sports chiropractic and rehabilitation. Dr. Danchik is an associate editor of the Journal of the Neuromusculoskeletal System. He has been in private practice in Massachusetts for 26 years. He can be reached by e-mail at