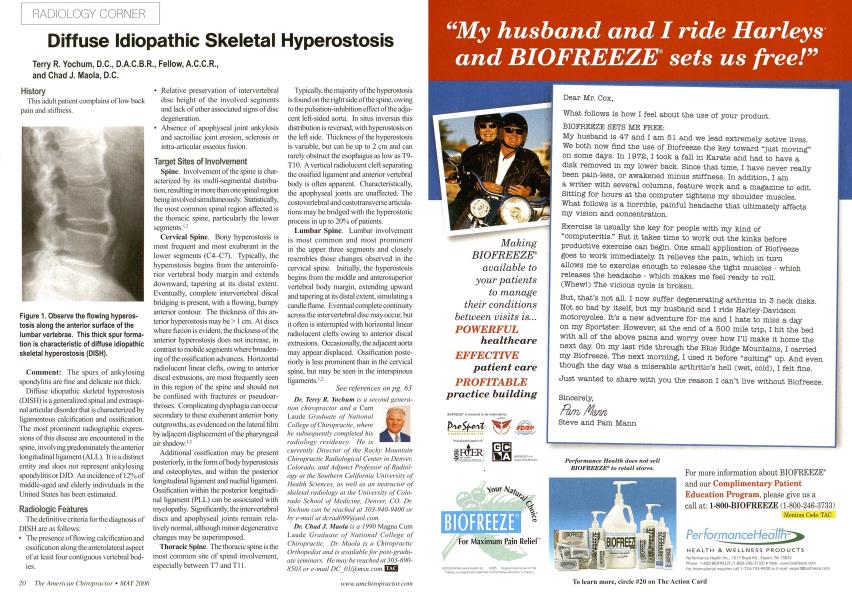
Terry R. Yochum, D.C., D.A.C.B.R., Fellow, A.C.C.R., and Chad J. Maola, D.C. History This adult patient complains of low back pain and stiffness. Comment: The spurs of ankylosing spondylitis are fine and delicate not thick. Diffuse idiupathic skeletal hypcrostosis (DISH) is a generalized spinal and extraspi-nal articular disorder that is characterized by ligamcntous calcification and ossification. The most prominent radiographic expressions of this disease are encountered in the spine, involving predominately the anterior longitudinal ligament (ALL). It is a distinct entity and does not represent ankylosing spondylitis or DJD. An incidence of 12% of middle-aged and elderly individuals in the United States has been estimated. Radiologic Features The definitive criteria for the diagnosis of DISH are as follows: • The presence of flowing calcification and ossification along the anterolateral aspect of at least four contiguous vertebral bodies. Relative preservation of intervertebral disc height of the involved segments and lack of other associated signs of disc degeneration. Absence of apophyscal joint ankylosis and sacroiliac joint erosion, sclerosis or intra-articular osseous fusion. Target Sites of Involvement Spine. Involvement of the spine is characterized by its multi-segmental distribution, resulting in more than one spinal region being involved simultaneously. Statistically, the most common spinal region affected is the thoracic spine, particularly the lower segments.1- Cervical Spine. Bony hyperostosis is most frequent and most exuberant in the lower segments (C4-C7). Typically, the hyperostosis begins from the anteroinfe-rior vertebral body margin and extends downward, tapering at its distal extent. Eventually, complete intervertebral discal bridging is present, with a flowing, bumpy anterior contour. The thickness of this anterior hyperostosis may be > 1 cm. At discs where fusion is evident, the thickness of the anterior hyperostosis does not increase, in contrast to mobile segments where broadening of the ossification advances. Horizontal radiolucent linear clefts, owing to anterior discal extrusions, are most frequently seen in this region of the spine and should not be confused with fractures or pseudoar-throses. Complicating dysphagia can occur secondary to these exuberant anterior bony outgrowths, as evidenced on the lateral film by adjacent displacement of the pharyngeal air shadow.1-2 Additional ossification may be present posteriorly, in the form of body hyperostosis and osteophytes, and within the posterior longitudinal ligament and nuchal ligament. Ossification within the posterior longitudinal ligament (PLL) can be associated with myelopathy. Significantly, the intervertebral discs and apophyseal joints remain relatively normal, although minor degenerative changes may be superimposed. Thoracic Spine. The thoracic spine is the most common site of spinal involvement, especially between T7 and Tl 1. Typically, the majority of the hyperostosis is found on the right side of the spine, owing to the pulsation-inhibition effect of the adjacent left-sided aorta. In situs inversus this distribution is reversed, with hyperostosis on the left side. Thickness of the hyperostosis is variable, but can be up to 2 cm and can rarely obstruct the esophagus as low as T9-T10. A vertical radiolucent cleft separating the ossified ligament and anterior vertebral body is often apparent. Characteristically, the apophyseal joints are unaffected. The costovertebral and costotransverse articulations may be bridged with the hyperostotic process in up to 20% of patients. Lumbar Spine. Lumbar involvement is most common and most prominent in the upper three segments and closely resembles those changes observed in the cervical spine. Initially, the hyperostosis begins from the middle and anterosuperior vertebral body margin, extending upward and tapering at its distal extent, simulating a candle flame. Eventual complete continuity across the intervertebral disc may occur, but it often is interrupted with horizontal linear radiolucent clefts owing to anterior discal extrusions. Occasionally, the adjacent aorta may appear displaced. Ossification posteriorly is less prominent than in the cervical spine, but may be seen in the interspinous ligaments.1-2 See references on pg. 63 Dr. Terry R. Yochum is a second genera- lion chiropractor and a Cum Laude Graduate of National College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology at the University of Colorado School of Medicine, Denver, CO. Dr. Yochum can be reached at 303-940-9400 or by e-mail at dcradO99(a aol.com. Dr. Chad J. Maola is a 1990 Magna Cum Laudc Graduate of National College of Chiropractic. Dr. Maola is a Chiropractic Orthopedist and is available for post-graduate seminars. He may be reached at 303-690-8503 or e-mail DC_Ol(w,msn.com.\ Figure 1. Observe the flowing hyperostosis along the anterior surface of the lumbar vertebrae. This thick spur formation is characteristic of diffuse idiopathic skeletal hyperostosis (DISH).