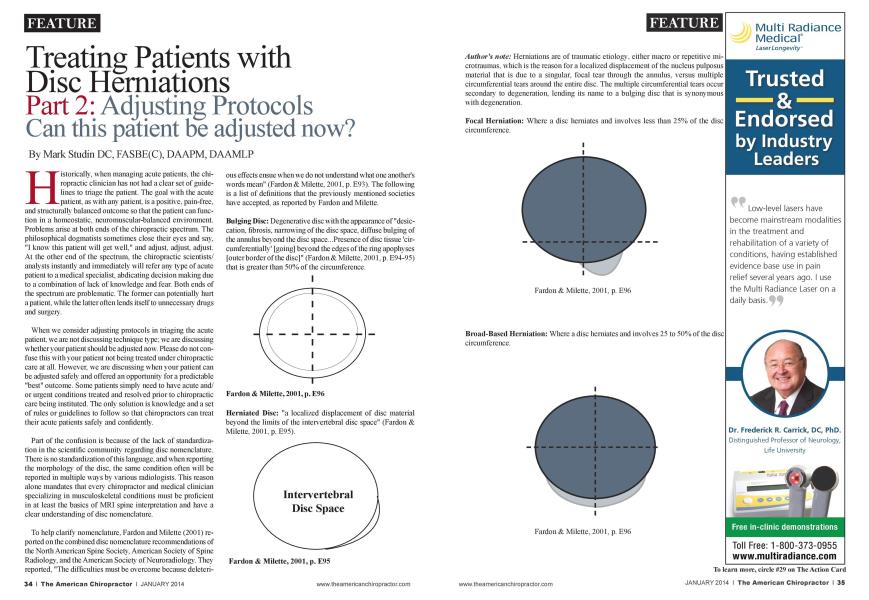
Historically, when managing acute patients, the chiropractic clinician has not had a clear set of guidelines to triage the patient. The goal with the acute patient, as with any patient, is a positive, pain-free, and structurally balanced outcome so that the patient can function in a homcostatic. ncuromuscular-balanccd environment. Problems arise at both ends of the chiropractic spectrum. The philosophical dogmatists sometimes close their eyes and say. "I know this patient will get well." and adjust, adjust, adjust. At the other end of the spectrum, the chiropractic scientists/ analysts instantly and immediately will refer any type of acute patient to a medical specialist, abdicating decision making due to a combination of lack of knowledge and fear. Both ends of the spectrum are problematic. The former can potentially hurt a patient, while the latter often lends itself to unnecessary dmgs and surgery. When we consider adjusting protocols in triaging the acute patient, we are not discussing technique type: we arc discussing whether your patient should be adjusted now. Please do not confuse this with your patient not being treated under chiropractic care at all. However, we arc discussing when your patient can be adjusted safely and offered an opportunity fora predictable "best" outcome. Some patients simply need to have acute and/ or urgent conditions treated and resolved prior to chiropractic care being instituted. The only solution is know ledge and a set of rules or guidelines to follow so that chiropractors can treat their acute patients safely and confidently. Part of the confusion is because of the lack of standardization in the scientific community regarding disc nomenclature. There is no standardization of this language, and when reporting the morphology of the disc, the same condition often w ill be reported in multiple ways by various radiologists. This reason alone mandates that every chiropractor and medical clinician specializing in musculoskclctal conditions must be proficient in at least the basics of MRI spine interpretation and have a clear understanding of disc nomenclature. To help clarify nomenclature. Fardon and Milcttc (2001) reported on the combined disc nomenclature recommendations of the North American Spine Society. American Society of Spine Radiology, and the American Society of Ncuroradiology. They reported. "The difficulties must be overcome because dclctcri- ous effects ensue when we do not understand what one another's words mean" (Fardon & Milcttc. 2001. p. E93). The following is a list of definitions that the previously mentioned societies have accepted, as reported by Fardon and Milette. Bulging Disc: Degenerative disc with the appearance of "desiccation, fibrosis. narrowing of the disc space, diffuse bulging of the annulus beyond the disc space...Presence of disc tissue 'cir-cumfcrcntially' [going] beyond the edges of the ring apophyscs | outer border of the disc]" (Fardon & Milette. 2001. p. E94-95) that is greater than 50% of the circumference. Hcrniatcd Disc: "a localized displacement of disc material beyond the limits of the intervertcbral disc space" (Fardon & Milette, 2001, p. E95). Author's note: Hcrniations arc of traumatic etiology, either macro or repetitive mi-crotraumas. which is the reason fora localized displacement of the nucleus pulposus material that is due to a singular, focal tear through the annulus. versus multiple circumferential tears around the entire disc. The multiple circumferential tears occur secondary to degeneration, lending its name to a bulging disc that is synonymous with degeneration. Focal Hcrniation: Where a disc hemiates and involves less than 25% of the disc circumference. Broad-Based Herniation: Where a disc hemiates and involves 25 to 50% of the disc circumference. Protrusion Type Hcrniatcd Disc: Is present "if the greatest plane, in any direction, between the edges of the disc material beyond the disc space is less than the distance between the edges of the base when measured in the same plain" (Far-don & Milettc. 2001. p. El00). Simply, the disc is wider at the base than the apex similar to a pyramid. Extrusion-Migration Type Hcrniatcd Disc: Is present when "in at least one plane, any one distance between the edges of the disc material beyond the disc space is greater than the distance between the edges of the base..." (Fardon & Milcttc. 2001. p. El00). Simply, the disc is wider at any point in the apex than it is at the base, similar to the shape of a mushroom. In the first part of this two-part scries titled "MRI Ordering Protocols." Studin (November. 2013) discussed the specific protocols, offering guidelines for when to order an MRI. He discussed triaging patients with consideration of radiculopathy. myclopathy. or the absence of both, and when to order an MRI. The chiropractic profession, similar to the orthopedic neurosurgeon or spine surgeon, practices its art in a manner that affects the spinal and contiguous neurological components. As a result, guidelines for making a prognosis and determining treatment plans arc focused on spinal neural comprcssivc components because of space-occupying lesions with the prime lesion being the disc. It is critical to understand that a complete and thorough clinical evaluation is mandatory in managing every patient, but more acute with the hcrniatcd disc patient. The clinical correlation between the examination and the MRI findings will be the arbiter of both your prognosis and treatment plan. It is also the determining factor in triaging your patient for cither a neurosurgical or pain management consultation. Therefore, a complete orthopedic and neurological evaluation is mandated, and if you perform a complete examination as you were taught going through professional doctoral training, you will be on firm ground as there is nothing esoteric in your clinical evaluation to help guide you. It is the application of simple motor, sensory, upper, and lower motor neuron lesion clinical testing. Two conditions help guide the triaging of your patient when determining adjusting protocols: Radiculopathy: Compression of a nerve root in the neural canal, neural foramen, or spinal canal below the conus mcdullaris. Myclopathy: Compression of the spinal cord with ensuing neurological deficit distal to the level of lesion. The reason radiculopathy and myclopathy are considered is because they are neuro-comprcssivc syndromes and quite simply, the proximity of the lesion to the neurological entity is the arbiter and basis for our guidelines on when to adjust. Another way to understand the issue is one of "real estate." Is there enough cerebral spinal fluid (also known as space or real estate) around the neurological entity to safely adjust your patient? These two conditions arc not only the arbiter for adjusting, they arc also the basis for immediate MRIs according to Fish. Kobayashi. Chang, and Pham (2009). and further indicate the necessity for MRI imaging studies prior to rendering an adjustment with these two patient populations based upon your clinical evaluation. The following MRI image is that of a normal cervical spinal cord in the axial plane. Please note, the adequate amount of space around the entire cord giving a clear indication, barring any other comorbidities that this patient is safe to adjust. Author's note: If you do not know how to understand the above axial cervical image, you must be educated at the \ cry least with the basics of MRI spine interpretation. We strongly suggest going to www .TcacliDoctors.com. In the aboYC picture, there is clearly enough cerebral spinal fluid or space around the spinal cord to safely adjust the patient. In the picture below, you will sec that there is no cerebral spinal fluid or space between the disc and spinal cord. However, there is what appears to be adequate space or cerebral spinal fluid on the posterior side between the cord and the liganicntum flavum. This is considered an effaccment of the disc on the cord and because there is a space-occupying lesion (disc) in contact with a neurological clement (spinal cord), the arbiter for adjusting this patient will be the clinical evaluation. The issue is how much negative neurological scqucllac the patient is experiencing with a focus on both motor and/or sensory deficit. This type of patient will usually respond well to chiropractic care with the proviso that a ncurosurgical consultation should be considered to ensure an accurate diagnosis, prognosis, and treatment plan. This type of patient often requires co-management. The following scenario would be considered a clear indication of the necessity for an immediate ncurosurgical consultation prior to considering a treatment plan that starts with a chiropractic adjustment because there is no cerebral spinal lluid (space or "real estate") on cither side of the cord. This is considered a cord compression and clearly an indication for an immediate referral for consideration of ncurosurgical intervention. Should there be neurological dchcit distal to the lesion, a myclopathy would be present. Author's note: The above cervical spinal cord issues arc only one example: the same applies for the nerve roots in both the neural canals throughout the spine and the central canal (cauda cquina and distributions) in the lumbar spine. This standard has helped create a guideline with predictable outcomes that lias been done in collaboration with Magdy Shady. MD. ncurosurgcon. ncurotrauma fellow for 23 years. Doctors have practiced these same standards nationally with thousands of patients who have been able to receive chiropractic care in a confident and safe environment. In most cases, chiropractic could be delivered with the proviso that some patients necessitated surgical intervention in urgent scenarios. Chiropractic care was delivered post-surgically while co-managed with the ncuro or spine surgeon. It is also critical to ensure that the spine surgeon is versed in chiropractic care in understanding both the delivery of chiropractic and the scientific literature reporting the positive outcomes of chiropractic intervention versus surgery in disc hcrniation patients. McMorland. Sutcr. Casha. du Plcssis. and Hurlbcrt (2010) found that 60% of surgical candidates had successful outcomes with chiropractic as an alternative to surgery. This type of scientific literature will help foster a collaborative relationship between the chiropractic and spine surgeon, and help prevent unnecessary surgeries. It is the role of the practicing chiropractor to educate the surgical community through the literature. One of the best ways for the chiropractic profession to spiral upward is through clinical excellence with our feet firmly planted in the basic principles of chiropractic. MRI spine interpretation and triaging the acute arc two areas that mandate clinical excellence for the entire chiropractic profession. References: 1. Studin. M. (2013). Treating patients with disc hcrnia-tions. Part 1: MRI ordering protocols. American Chiropractor. 35(11). 28. 30. 32. 33 2. Fardon D.. & Milcttc P. (2001). Nomenclature and clas- sification of lumbar disc pathology. Recommendations of the Combined Task Forces of the North American Spine Society of Spine Radiology, and American Society of Ncuroradiology. Spine. 26(5). E93-E113. Fish. D. E.. Kobayashi. H. W.. Chang. T. L.. & Pham. Q. (2009). MRI prediction of therapeutic response to epidural steroid injection in patients with cervical ra-diculopathy. American Journal of Physical Medicine & Rehabilitation. 88(3). 239-246. McMorland. G.. Suter. E.. Caslia. S.. du Plcssis. S. J.. & Hurlbcrt. R. J. (2010). Manipulation or microdisccctomy for sciatica? A prospective randomized clinical study. Journal of Manipulative and Physiological Therapeutics, 33(8). 576-584. Dr. Mark Studin is an adjunct assistant professor in clinical sciences at the University of Bridgeport College of Chiropractic and a clinical presenter for the State of New York at Buffalo, School of Medicine and Hiomedical Sciences for post-doctoral education, teaching MM spine interpretation and triaging trauma cases. lie is also the president of the Academy of Chiropractic teaching doctors of chiropractic how to interface with the legal community (www. LawyersPIProgram.com) and teaches A/RI interpretation and triaging trauma cases to doctors of all disciplines nationally (www.TeachDoctors.com). He can be reached at DrMark@ TeachDoctors.com or at 631-786-4253.