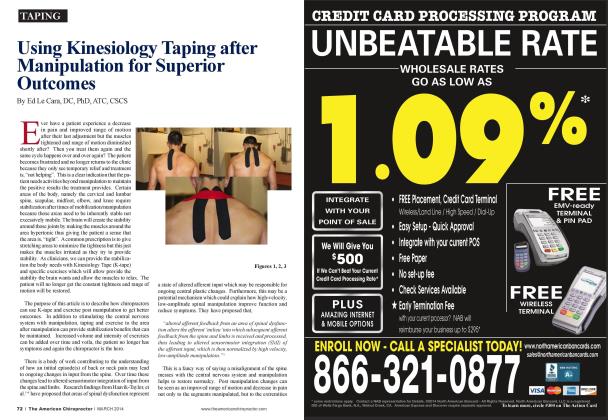
T here are two shoulder orthopedic tests performed in the functional movement screen (FMS). These two tests are called clearing/qualifying tests when performed along with the shoulder mobility screen. (Photo 1) The shoulder mobility screen assesses bilateral shoulder range of motion, combining internal rotation with adduction and external rotation with abduction. The shoulder mobility screen also requires normal scapular mobility and thoracic spine extension. The tester first determines the hand length by measuring (with a tape measure or marked dowel) the distance from the distal wrist crease to the tip of the third digit in inches. The patient is then instructed to make a fist with each hand, placing the thumb inside the fist. The patient is then asked to assume a maximally adducted. extended, and internally rotated position with one shoulder and a maximally abducted. Hexed, and externally rotated position with the other. During the test, the hands should remain in a fist and they should be placed on the back in one smooth motion. The tester then measures the distance between the two closest bom prominences. The shoulder mobility test is then scored per the FMS criteria (a scale of 0 to 3). The "clearing" tests are shoulder "internal rotation and adduction" and shoulder "horizontal adduction." Placing the right palm and fingers on the top of the left shoulder and elevating the elbow to the forehead is also known as the Mazion shoulder maneuver. (Photo 2) We consider this a positive test (+) if discomfort is intensified and/or there is localized pain in the shoulder. Placing the hand on the opposite shoulder and touching the elbow to the chest is know n as the Dugas test, and if there is (+) pain and/or inability to perform the movement, then it indicates dislocation of the shoulder. Another part of the shoulder screen is taking the right arm horizontally across the chest (moving the right arm leftward) and pulling the ami further with the left hand. This is called cross chest adduction or the forced adduction test. To accomplish this movement, the client first abducts the ami to 90 degrees and then moves the arm across the front of the body. The arm flexed to 90 degrees is adducted forcibly across the chest with the opposite hand. Pain with this test indicates subcoraeoid impingement and/or acromioclavicular joint impingement. The pinching of any stmcture between the head of the hu-merus and the acromion is referred to as impingement of the shoulder. This may include the bursa. the rotator cuff tendons, or the tendon of the long head of the biceps brachii muscle. It is theorized that impingement is caused by a superior and anterior glide of the humeral head in the glenoid fossa. This causes the greater tubercle to approximate the acromion process and impinge the tissues between them (supraspinatus tendon, subacromial bursa. long head of the biceps tendon, anterior capsule). For example, an individual with ovcractivc deltoids (in particular the posterior deltoid), supraspinatus. and coracobra-chialis will experience excessive superior and anterior migration of the humcrus during shoulder abduction and/or flexion. These clearing tests don"t tell us what the thoracic spine looks like, or what the scapular motion is or is not doing as it pertains to impairment. We still have to do a visual posture analysis. We need to observe the clients movement during all phases of screening for any limitation of motion or any break of normal rhythm or symmetry. Scapular winging is a common impairment and easily visualized. If you have a winged scapula, (scapular winging) the entire vertebral border of the scapula protnidcs posteriorly from the thorax (the shoulder blade will stick out). Because the scapula is pulled away from the ribcage. it renders the scrratus anterior relatively long and this means the scrratus anterior muscle is most likely weak. A strong scrratus anterior suctions your scapula in against the ribcage during movement, which eliminates the winged look. The scrratus anterior muscle often needs activation exercise. There are many scr-ratus anterior exercises used to treat various upper-body pathologies. The serratus is particularly effective for improving scapulohumeral rhythm as an upward rotator of the scapula. In general, scapular winging indicates poor shoulder girdle stability and control and an undcractivc/long serratus anterior. Thoracic kyphosis is an increased outward (posteriorly orientated) curve or flexion of the thoracic spine. Kyphosis is very common and an easily visualized dysfunction. As we sit more often and get older, people adopt more sedentary lifestyles that lead to thoracic kyphosis. The problem is when the kyphotic curve becomes increased and it is associated with stiffness. The thoracic spine is naturally the stiffest section of the spine because of the rib attachments forming the costotransverse and costovcrtcbral joints. The two main planes of thoracic movement arc llexion/ extension and rotation. We test thoracic spine motion several times in the selective functional movement assessment (SFMA) and FMS. During the FMS. the squat, the in-line lunge, shoulder mobility, push-up test, and rotary stability test. In the SFMA. we test thoracic mobility in the two shoulder tests (elbow elevation test and the cross shoulder adduction test), trunk rotation, and the squat. I like to think of the thoracic spine in three sections: upper thoracic spine, which has a very important relationship to the neck, the mid thoracic spine, and the thoraeolunibar junction, which lias a very important relationship to the lower back. Kyphosis can occur at any of these sections. So it is important to assess exactly where the stiffness is taking place. The current corrective exercise progression for shoulder dysfunction is to treat from proximal to distal. This means that you check the core before working on what's going on with the extremities. Why stretch a tight shoulder if you haven't taken into consideration where the ccrvicothoracic and thoracic spine is positioned? Start with the thoracic spine and the latissimus dorsi restrictions. Foam roll the thoracic spine by using the foam roller or KnotOut (LavitaFortc.com) and laying it cross the spine in the most restricted area, with the knees bent up. and then arch the back over the restricted area. This is a useful flexibility exercise. In addition, pcrfomi quadruped range of movement exercises, such as "thread the needle." aimed at increasing movement of the joints that make up the thoracic spine. Any thoracic spine flexibility exercise into rotation, flexion, and particularly extension are essential. Other first-line flexibility exercises would include stretches for the pecs and lats. Tightness through the pecs and lats can often pull the shoulders forward and increase the kyphosis. If someone has a positive impingement test, look for stiffness in the thoracic spine, and/or rounded shoulders through the thoracic spine. The rhomboids, leva-tor scapulae, and upper trapezius (sometimes ovcractivc. sometimes undcractivc) muscles arc often very tight and ovcrac-tivc. Performing self myofascial release, trigger point therapy, and stretching of these muscles may change the positive impingement test. Other muscles that hold the thoracic spine and scapula in correct posture include the lower trapczius. serratus anterior, and thoracic erector spinac. Some useful exercises to help improve their function are back extension, rows, and upward diagonal band/cable pulls. The "push-up plus" (Photo 3) is often used to improve serratus anterior function. Another common exercise is the Ys. Ts. and Ws. You have your feet on the ground and up against the w all face down with a stability ball positioned under your stomach and pelvis. You have to hold your thoracic spine extended while feeling like you arc pushing your chest out and pulling shoulders away from your cars. Then make the letters Y. T. and W with your arms and hold each position for 10 seconds. This exercise should be prescribed on a case-by-case basis. I hope this helps you with clients suffering from impingement related to thoracic kyphosis. If it doesn't make a change, there may be a glenohumeral problem and this will take further evaluation. References: Silliman JF. Hawkins RJ: Clinical Examination of the Shoulder Complex. In Andrews JR. WillkKE (eds): The Athlete's Shoulder. New York. Churchill Livingstone. 1994. www.FunctionalMovemcnt.com Dr. Jeffrey Tucker is the 2012 ACA Rehab Council Doctor of the Year. He is the ACA Rehab Council Secretary Treasurer and a certified instructor for the Functional Movement Screen (FMS) workshops. He is also on the education committee for the Ilygenic Corporation, and is a postgraduate instructor for the diploniale program offered by the American Chiropractic Rehabilitation Board. 1 hit his website at www.Dr.IeffreyTucker.com