ABDOMINAL AORTIC ANEURYSM
RADIOLOGY CORNER
Terry R. Yochum
D.C., D.A.C.B.R., Fellow, A.C.C.R.,
Alicia M. Yochum
D.C., R.N., BSN
HISTORY:
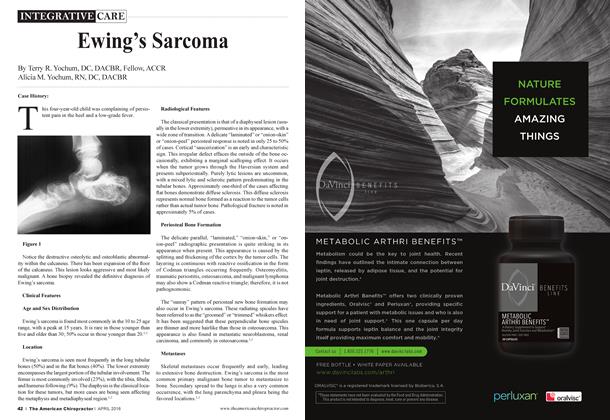
Two adult patients present with nonspecific lower back pain. Figure 1 is a plain film radiograph of the abdomen (without contrast injection) where clearly defined calcification of the abdominal aorta with aneurysmal dilatation of the aorta is identified. Figure 2 represents a contrast examination of the aorta where there is extensive dilatation of the vascular structure.
DISCUSSION:
An aneurysm is a localized abnormal dilatation of any vessel. Aneurysms may occur in any artery or vein in the body and are classified according to location, etiology and gross appearance.
Location: The most comm ou sites of involvement in order of frequency are the aorta, iliac, splenic, renal and intracranial arteries.
Etiology: Aneurysms are either congenital or acquired. For the purpose of this discussion, we will only deal with acquired aneurysms associated with aging and degenerative atherosclerosis.
The aorta is the most common vessel to develop an aneurysm. The leading cause is atherosclerosis. Greater than 95% of atherosclerotic aneurysms occur between 60 and 80 years of age. Men aie affected four times more commonly than women. The most common locations within the aorta for aneurysm formation in order of incidence are the abdominal aorta, aortic arch, descending thoracic aorta and rarely the ascending aorta associated with syphilis.
Abdominal Aorta: The radiological depiction of an aortic aneurysm is best evaluated with frontal, lateral and oblique radiographs. Most abdominal aortic aneurysms occur between the renal artery (L2) and iliac bifurcation (L4), and this is the key region to evaluate. The aneurysm itself will be visible as a soft tissue density often demarcated by thin, curvilinear rim of continuous or discontinuous calcification. It is this calcification which usually confirms the diagnosis but is only present in just
over 50% of cases. On the frontal AP projection, the majority of the lesion is to the left of the midline. On the lateral view, the aorta usually expands anteriorly but occasionally may develop a posterior extension. An aneurysm is present if the diameter of the aorta is greater than 3.8 cm. This measurement is made on a lateral radiograph horizontally, between the most distant calcified borders. A measurement of 5.5 cm is usually an indication for surgical intervention. Those lesions greater than 6 cm are prone to rupture in over 50% of cases. The diagnostic modality of choice for definitive diagnosis is diagnostic ultrasound, which will confirm the diagnosis, evaluating the size of the aorta and monitoring progression or stability.
In the presence of an aneurysm and appropriate clinical signs of abdominal pain and falling blood pressure, obliteration of the psoas margin on a recumbent film may be a sign of dissection leaking into the peritoneal cavity.
The close proximity of the aorta to the anterior vertebral bodies infrequently precipitates extrinsic anterior erosion (Oppenheimer erosions) due to the increased transmission of the aortic pulse. These defects are smooth and concave, with the disc endplate region being relatively unaffected. Other causes of anterior body defects include lymphoma, lytic metastasis and subligamentous tuberculosis.
PROGNOSIS:
Patients who dissect and rupture their abdominal aortic aneurysms have a prognosis of 95% fatality with only 5% surviving. Patients with an abdominal aortic aneurysm who have elective abdominal surgery have a 5% mortality rate with 95% survival rate.
Dr. Terry R. Yochum is a second generation chiropractor and a Cum Laude Graduate of National College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology at the University of Colorado School of Medicine, Denver, CO. Dr. Yochum can be reached at 1-303-940-9400 or by e-mail at [email protected]
Dr. Alicia M. Yochum is a third generation chiropractor and 2011 Suma Cum Laude Graduate of Logan College of Chiropractic, as well as a Registered Nurse. She is in a Radiology residency at Logan College in St. Louis, MO. She can be reached at [email protected].
REFERENCES:
1. Yochum TR, Rowe LJ: Essentials of Skeletal Radiology, ed 3. Baltimore, Williams & Wilkins, 2005.