Ewing’s Sarcoma
INTEGRATIVE CARE
Terry R. Yochum
DC, DACBR, Fellow, ACCR
Alicia M. Yochum
RN, DC, DACBR
Case History:
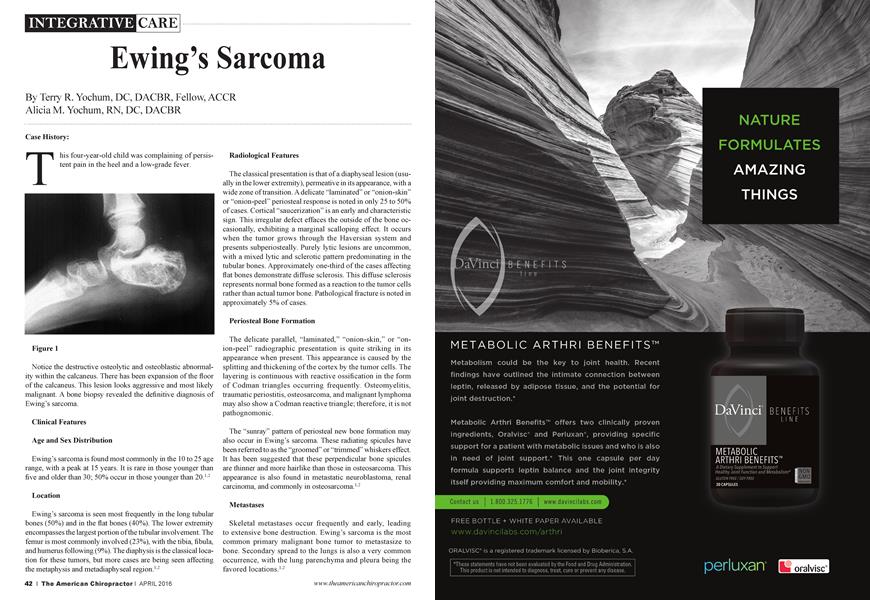
This four-year-old child was complaining of persistent pain in the heel and a low-grade fever.
Notice the destinctive osteolytic and osteoblastic abnormality within the calcaneus. There has been expansion of the floor of the calcaneus. This lesion looks aggressive and most likely malignant. A bone biopsy revealed the definitive diagnosis of Ewing’s sarcoma.
Clinical Features
Age and Sex Distribution
Ewing’s sarcoma is found most commonly in file 10 to 25 age range, with a peak at 15 years. It is raie in those younger than five and older than 30; 50% occur in those younger than 20.12
Location
Ewing’s sarcoma is seen most frequently in the long tubular bones (50%) and in the flat bones (40%). The lower extremity encompasses the largest portion of the tubular involvement. The femur is most commonly involved (23%), with the tibia, fibula, and humerus following (9%). The diaphysis is the classical location for these tumors, but more cases aie being seen affecting the metaphysis and metadiaphyseal region.12
Radiological Features
The classical presentation is that of a diaphyseal lesion (usually in the lower extremity), permeative in its appearance, with a wide zone of transition. A delicate “laminated” or “onion-skin” or “onion-peel” periosteal response is noted in only 25 to 50% of cases. Cortical “saucerization” is an early and characteristic sign. This irregular defect effaces the outside of the bone occasionally, exhibiting a marginal scalloping effect. It occurs when the tumor grows through the Haversian system and presents subperiosteally. Purely lytic lesions aie uncommon, with a mixed lytic and sclerotic pattem predominating in the tubular bones. Approximately one-third of the cases affecting flat bones demonstrate diffuse sclerosis. This diffuse sclerosis represents normal bone formed as a reaction to the tumor cells rather than actual tumor bone. Pathological fracture is noted in approximately 5% of cases.
Periosteal Bone Formation
The delicate parallel, “laminated,” “onion-skin,” or “onion-peel” radiographic presentation is quite striking in its appearance when present. This appearance is caused by the splitting and thickening of the cortex by the tumor cells. The layering is continuous with reactive ossification in the form of Codman triangles occurring frequently. Osteomyelitis, traumatic periostitis, osteosarcoma, and malignant lymphoma may also show a Codman reactive triangle; therefore, it is not pathognomonic.
The “sunray” pattem of periosteal new bone formation may also occur in Ewing’s sarcoma. These radiating spicules have been referred to as the “groomed” or “trimmed” whiskers effect. It has been suggested that these perpendicular bone spicules aie thinner and more hairlike than those in osteosarcoma. This appearance is also found in metastatic neuroblastoma, renal carcinoma, and commonly in osteosarcoma.12
Metastases
Skeletal metastases occur frequently and early, leading to extensive bone destruction. Ewing’s sarcoma is the most common primary malignant bone tumor to metastasize to bone. Secondary spread to the lungs is also a very common occurrence, with the lung parenchyma and pleura being the favored locations.12
■ "Ewing’s sarcoma is the most common primary malignant bone tumor to metastasize to bone. ï Ï
Treatment and Prognosis
The five-year survival rate has been approximately 5% for Ewing’s sarcoma. Radiation therapy rendered in conjunction with effective chemotherapy in lesions detected early is increasing the survival rate. Amputation may still be used in lesions around the knee. A recent study reports a 35% five-year survival rate in 107 patients. Early detection remains the key to effective treatment and improved prognosis.12
References:
1. Yochum TR, Rowe LJ: The Essentials of Skeletal Radiology, 3rd ed., Baltimore, Williams & Wilkins, 2005.
2. Re snick D: Diagnosis of Bone and Joint Disorders, ed. 4, Philadelphia, WB Saunders, 2002.
0Dr. Terry R. Yochum is a second-generation chiropractor and a cum laude graduate of the National College of Chiropractic, where he subsequently completed his radiology specialty. He is a Diplomate of the American Chiropractic Board of Radiology and served as its Vice-President and President for seven years (1983-1990). Dr. Yochum is currently the Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado. On September 27,1996Dr. Yochum was bestowed the honor of "Fellow " by the American Chiropractic College of Radiology (ACCR). He is the youngest recipient ever to receive this award, which has only been given to eight DACBR ’s since the inception of the ACCR in 1958. Dr. Yochum has been inducted into 4 Hall Of Fames. Dr. Terry Yochum can be contacted at dcrad099(f aol.com.
H Alicia M. Yochum RN, DC, DACBR received her Bachelor of Science in Nursing from Point Loma Nazarene University and then worked in the ICUfor one year before matriculating to Logan College of Chiropractic where she graduated Sum Cum Laude in 2011. She completed her diagnostic imaging residency at Logan in 2015 and received her DACBR in October of 2015 becoming the first second generation DACBR in the history of chiropractic. She has performed editorial review for the Journal of Chiropractic Medicine and she serves as an Associate Editor for the Journal of the Academy of Chiropractic Orthopedics (JACO). Dr. Yochum has published many articles in peer reviewedjournals and lectured around the country with her father, Dr. Terry R Yochum, as well as in England and Germany. She is currently completing her fellowship in musculoskeletal advanced imaging at Logan University with an emphasis on musculoskeletal diagnostic ultrasound. Dr. Alicia Yochum can be contacted at alicia.yochum a gmail.com.