Sports Medicine Insights Understand - Rehabilitate - Prevent
David Cruz
Help patients prevent low back pain through exercise programming.
The economic impact of low back pain (LBP) is greater than $100 billion per year and causes more disability globally than any other condition.1,2 It is the most common cause of activity limitation in adults age 45 and younger, and only second to arthritis in people age 45 to 65.3 Of those who suffer an episode of LBP, approximately 50% will experience a recurrence by year one, 60% by year two, and 70% by year five.4 Given this economic and societal burden, a considerable amount of effort has gone into understanding the cause, treatment, and prevention of this global problem.
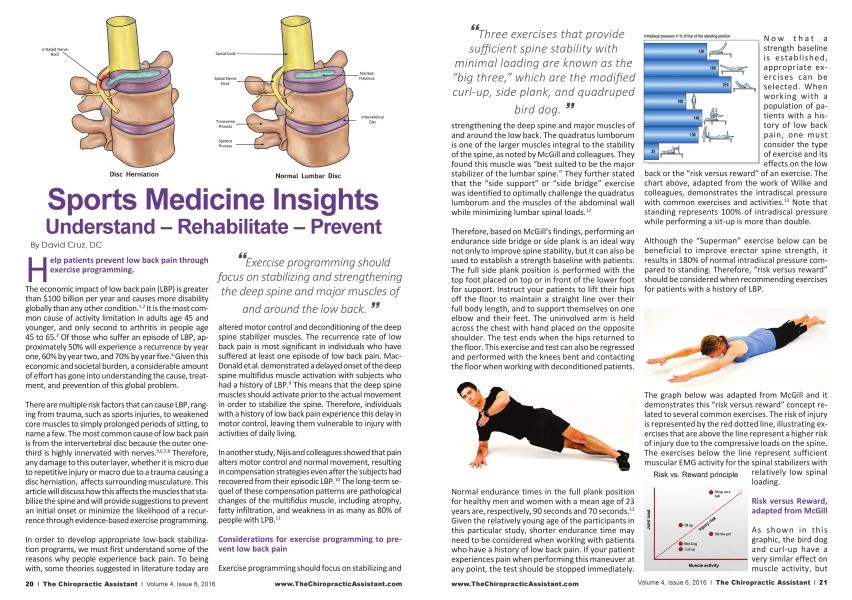
There are multiple risk factors that can cause LBP, ranging from trauma, such as sports injuries, to weakened core muscles to simply prolonged periods of sitting, to name a few. The most common cause of low back pain is from the intervertebral disc because the outer onethird is highly innervated with nerves.5'6'78 Therefore, any damage to this outer layer, whether it is micro due to repetitive injury or macro due to a trauma causing a disc herniation, affects surrounding musculature. This article will discuss how this affects the muscles that stabilize the spine and will provide suggestions to prevent an initial onset or minimize the likelihood of a recurrence through evidence-based exercise programming.
In order to develop appropriate low-back stabilization programs, we must first understand some of the reasons why people experience back pain. To being with, some theories suggested in literature today are
tk'Exercise programming should focus on stabilizing and strengthening the deep spine and major muscles of
and around the low back. 33
altered motor control and deconditioning of the deep spine stabilizer muscles. The recurrence rate of low back pain is most significant in individuals who have suffered at least one episode of low back pain. MacDonald et al. demonstrated a delayed onset of the deep spine multifidus muscle activation with subjects who had a history of LBP.9 This means that the deep spine muscles should activate prior to the actual movement in order to stabilize the spine. Therefore, individuals with a history of low back pain experience this delay in motor control, leaving them vulnerable to injury with activities of daily living.
In another study, Nijis and colleagues showed that pain alters motor control and normal movement, resulting in compensation strategies even after the subjects had recovered from their episodic LBP.10 The long-term sequel of these compensation patterns are pathological changes of the multifidus muscle, including atrophy, fatty infiltration, and weakness in as many as 80% of people with LPB.11
Considerations for exercise programming to prevent low back pain
Exercise programming should focus on stabilizing and
“ïhree exercises that provide sufficient spine stability with minimal loading are known as the "big three/' which are the modified curl-up, side plank, and guadruped
bird dog. 99
strengthening the deep spine and major muscles of and around the low back. The quadratus lumborum is one of the larger muscles integral to the stability of the spine, as noted by McGill and colleagues. They found this muscle was "best suited to be the major stabilizer of the lumbar spine." They further stated that the "side support" or "side bridge" exercise was identified to optimally challenge the quadratus lumborum and the muscles of the abdominal wall while minimizing lumbar spinal loads.12
Therefore, based on McGill's findings, performing an endurance side bridge or side plank is an ideal way not only to improve spine stability, but it can also be used to establish a strength baseline with patients. The full side plank position is performed with the top foot placed on top or in front of the lower foot for support. Instruct your patients to lift their hips off the floor to maintain a straight line over their full body length, and to support themselves on one elbow and their feet. The uninvolved arm is held across the chest with hand placed on the opposite shoulder. The test ends when the hips returned to the floor. This exercise and test can also be regressed and performed with the knees bent and contacting the floor when working with deconditioned patients.
Normal endurance times in the full plank position for healthy men and women with a mean age of 23 years are, respectively, 90 seconds and 70 seconds.12 Given the relatively young age of the participants in this particular study, shorter endurance time may need to be considered when working with patients who have a history of low back pain. If your patient experiences pain when performing this maneuver at any point, the test should be stopped immediately.
[\| Q yy that 3 strength baseline is established, appropriate exercises can be selected. When working with a population of patients with a history of low back pain, one must consider the type of exercise and its effects on the low
back or the "risk versus reward" of an exercise. The chart above, adapted from the work of Wilke and colleagues, demonstrates the intradiscal pressure with common exercises and activities.13 Note that standing represents 100% of intradiscal pressure while performing a sit-up is more than double.
Although the "Superman" exercise below can be beneficial to improve erector spine strength, it results in 180% of normal intradiscal pressure compared to standing. Therefore, "risk versus reward" should be considered when recommending exercises for patients with a history of LBP.
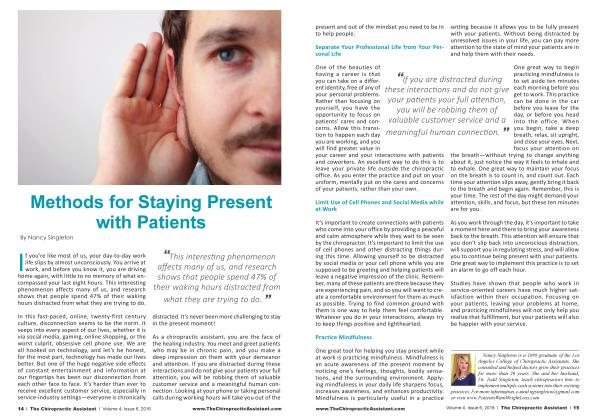
The graph below was adapted from McGill and it demonstrates this "risk versus reward" concept related to several common exercises. The risk of injury is represented by the red dotted line, illustrating exercises that are above the line represent a higher risk of injury due to the compressive loads on the spine. The exercises below the line represent sufficient muscular EMG activity forthe spinal stabilizers with Risk vs. Reward principle relatively low spinal
loading.
Risk versus Reward, adapted from McGill
As shown in this graphic, the bird dog and curl-up have a very similar effect on muscle activity, but
the sit-up has high spinal loading. The same holds true for the exercises "stir the pot" (low risk, high reward) and "sit up on a ball" (high risk, high reward). When developing generic protocols to prevent low back pain, it is safer to focus on integrating exercises that are below the "injury risk line" and are focused on low exercise volume.
Bird Dog Exercise-Activate core muscles. Raise one arm to shoulder level as opposite leg simultaneously lifts off floor, extendingto hip height. Pause momentarily. Return to start position and alternate sides. Maintain a straight spine position, not allowingyour hips to twist or rotate. Do not hyperextend low back when extending leg.
Three exercises that provide sufficient spine stability with minimal loading are known as the "big three," which are the modified curl-up, side plank, and quadruped bird dog. Spine stability requires muscles to be co-contracted for durations with relatively low levels of contractions. These exercises are designed for endurance and motor control and not for strength.14
McGill Curl-up - Lift shoulders off floor, trying to maintain a neutral spine position without rounding low back. Do not allow head to move forward of shoulders during movement. Elbows can remain in contact with floor during movement. Pause momentarily. Return to start position.
When performing these and other exercises to improve core stability, abdominal bracing or activation of the abdominal wall musculature is also recommended. These exercises should be performed in a neutral spine position when possible, avoiding pelvis tilting and excessive low back rounding or arching. After the patients have demonstrated sufficient strength and motor control, they may be progressed to exercises that involve flexion and extension in ordertofurtherstrengthentheabdominal and erector spinae musculature.15
Stir the pot - Begin kneeling in front of stability ball. Rest elbows on ball. Straighten legs into a plank
“As with oil exercise programs, long-term adherence and exercise execution on a regular basis are important to achieve satisfying
results.39
position. Keeping spine straight, roll elbows in a circular motion on the ball. Perform this movement in 10-second intervals resting three seconds in between reps.
Here are some general guidelines for working with patients with previous or existing low back conditions16:
• Never exercise through pain.
• Groove appropriate and perfect motion and motor patterns before adding load or other challenges.
• Start by taking gravity out of the equation—start supine or prone, quadruped, kneeling, then standing.
• Increase intensity or time, but not both.
• Intensity can be increased by either changing resistance or changing stability.
• If the patient is ready to be progressed, the following guidelines will help you do this safely and effectively17:
• If the patient is still making progress, continue with the current workload.
• If the patient is at plateau, progress at a 2 to 10% increase.
• If the patient experiences flare-ups, decrease volume.
Some other suggestions to consider when working with patients who have a history of LBP are:
• Avoid unsupported forward flexion exercises at first.
• Avoid lifting both legs in a supine or prone position.
• Avoid rapid movements, especially twisting at the waist.
• Extend warm-up and cool-down periods.
• Focus on good form, trainingthe movement and not the muscles.
As with all exercise programs, long-term adherence and exercise execution on a regular basis are important to achieve satisfying results. After the patients have mastered the movements and are able to maintain good form, they can be tasked with short
at-home protocols in forms of print outs or videos that will help them doing the exercises on their own. It is typically recommended to give patients protocols for two to four weeks. Ideally, they should come back to the office after the completion of this to recheck their form and to learn the appropriate exercise progressions. Regular check-ins and exercise progressions will also increase program adherence and long-term results.
References
1. Hoy, D., et ol. 2014 The global burden of low back pain: estimates from the Global Burden of Disease 2010 study.
2. Crow, W., Willis, D. 2009. Estimating cost of care for patients with acute low back pain: a retrospective review of patient records. J Am Osteopath Assoc. 2009 Apr;109(4):229-33.
3. Loney, P., Stratford, P. 1999. The Prevalence of Low Back Pain in Adults: A Methodological. Review of the Literature. Physical Therapy. Vol 79(4):384-396.
4. Hoy, D., et al. 2010. The Epidemiology of Low Back Pain. Best Practice and Research Clinical Rheumatology. 24:769-781.
5. Zhang, Y., et al. 2009. Clinical diagnosis for discogenic low back pain. Int. J. Biol. Sci. 5(7):647-658
6. Bogduk, N., et al. 2013. Lumbar Discogenic Pain: State-ofthe-Art Review. Pain Medicine. 14: 813-836.
7. Delitto, A., et al. 2012. Low Back Pain Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 42(4).
8. Hancock, M., et al. 2007. Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. Eur Spine J. 16:1539-1550.
9. MacDonald, D., et al. 2009. Why do some patients keep hurting their back? Evidence of ongoing back muscle dysfunction during remission from recurrent back pain. PAIN 142, 183-188.
10. Nijis, J., et al. 2012. Nociception Affects Motor Output, A Review on Sensory-motor Interaction With Focus on Clinical Implications. Clin J Pain Volume 28, Number 2.
11. Danneels, L., et al. 2001. Effects of three different training modalities on the cross sectional area of the lumbar multifidus muscle in patients with chronic low back pain. BrJ Sports Med 35:186-191.
12. McGill, S., et al. 1999. Endurance Times for Low Back Stabilization Exercises: Clinical Targets for Testing and Training From a Normal Database. Arch Phys Med Rehabil Vol 80.
13. Wilke, H., el al. 1999 New In Vivo Measurements of Pressures in the Intervertebral Disc In Dally Life. Spine. Vol24, Number 8, pp 755-762.
14. McGill, S. 2010. Core Training: Evidence Translating to Better Performance and Injury Prevention. Strength and Conditioning Journal. Vol 32(3).
15. Akuthota, V., et al. 2008. Core Stability Exercise Principles. Curr. Sports Med. Rep., Vol. 7(1) 39-44.
16. Adapted from Blog by Ed LeCara, PhD, DC, MBA, ATC, CSCS.
17. Med Sei Sports Exerc. 2009 Mar;41(3):687-708.
David Cruz, DC, CSCS, SFMA, CES has practiced as a sports chiropractor for 18 years. In 2005 his background in sports medicine and interest in technology lead him to start WebExercises in order to help patients and clients be more successful with their
exercise and rehab programs, www.webexercises.com