Anatomy of Joint Pain
CLINICAL
EXCELLENCE
Craig F. Buhler
Joint pain is one of the most common symptoms people experience. Remedies and treatments are as varied as the sources that promote them. These treatments merely address the symptom of pain without addressing the cause. Pain is seen as something to avoid rather than something to be valued. Many people are forced to curtail their favorite activities because of intense pain. The alternative is to ingest prescription drugs so these activities can be continued without pain.
NSAIDs are the most effective and commonly prescribed class of drugs in the United States, with between 70 and 75 million NS AID prescriptions written annually at a cost of approximately $2 billion.1'7 It has been estimated that 30 million people worldwide consume these drugs.8 Adverse NSAIDinduced GI events ranging ffom dyspepsia to severe complications that can lead to hospitalization, surgery, and death are reported more commonly than adverse effects from any other class of drags. These events represent a substantial economic burden to society and have well-documented negative effects on quality of life. Other adverse effects include renal dysfunction, hepatic dysfunction, dermatologic reactions, and drag/ drag interactions.9'13
Effective pain relief removes the alarm of pain but sup-
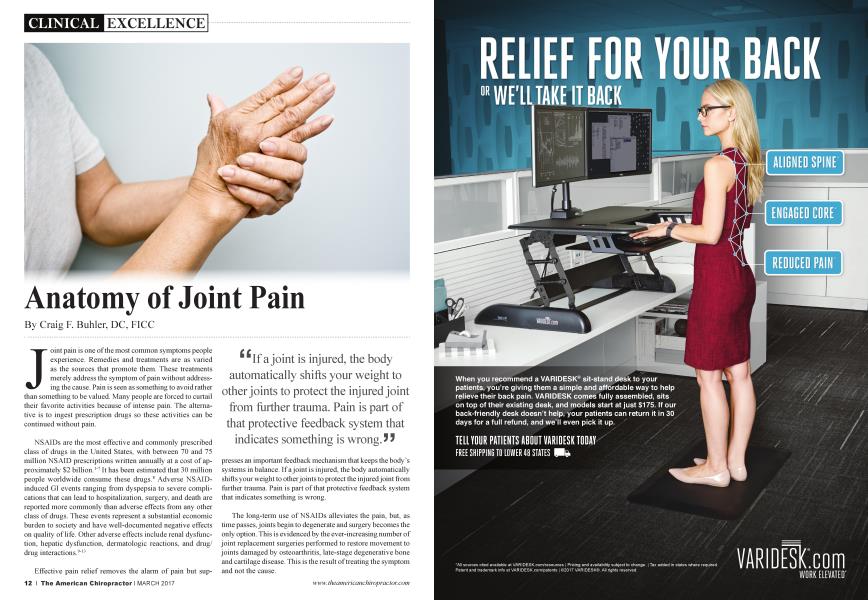
“If a joint is injured, the body automatically shifts your weight to other joints to protect the injured joint from further trauma. Pain is part of that protective feedback system that indicates something is wrong. J J
presses an important feedback mechanism that keeps the body’s systems in balance. If a joint is injured, the body automatically shifts your weight to other joints to protect the injured joint ffom further trauma. Pain is part of that protective feedback system that indicates something is wrong.
The long-term use of NSAIDs alleviates the pain, but, as time passes, joints begin to degenerate and surgery becomes the only option. This is evidenced by the ever-increasing number of joint replacement surgeries performed to restore movement to joints damaged by osteoarthritis, late-stage degenerative bone and cartilage disease. This is the result of treating the symptom and not the cause.
The number and rate of total hip replacements among inpatients age 45 and older increased from 138,700 in 2000 to 310,800 in 2010, or from a rate of 142.2 to 257.0 per 100,000 population. In the 10-year period from 2000 through 2010, an estimated 5.2 million total knee replacements were performed. Adults age 45 and older comprised 98.1% of those surgeries.14'15
It is the opinion of the author that the majority of hip and knee replacement surgeries are the result of chronic joint instability due to muscle inhibition caused by injuries managed with drugs. Muscle inhibition leads to tendon pain and conditions such as patellar tendonitis. Patellar tendonitis or jumpers knee is a frustrating clinical condition for patients and physicians alike. The disorder is common in athletes participating in
Symptoms are severe enough to force retirement in more than 50% of competitive athletes (Kettunen et al., 2002), and the injury represents over 15% of all soft-tissue injuries seen among military recruits during basic training. 5 J
jumping sports, such as volleyball (44%) and basketball (32%), and the incidence approaches 22% in the overall athletic population (Lian et al., 2005). Symptoms are severe enough to force retirement in more than 50% of competitive athletes (Kettunen et al., 2002), and the injury represents over 15% of all soft-tissue injuries seen among military recruits during basic training (Linenger et al., 1992). Jumper’s knee is an insertional tendinopathy that most commonly affects the patellar tendon origin on the inferior pole of the patella; it is not an inflammatory condition but a degenerative one.16'19
In a 15-year outcome study to study the prognosis of jumper’s knee comparing athletes with jumper’s knee and nonsymptomatic athletes, it was revealed that 53% of the subjects in the jumper’s knee group had to quit their sports career because of knee problems compared with 7% of the control subjects. The results of a follow-up study showed that jumper’s knee causes mild but long-lasting symptoms that remain after the athletic career is over. Cook and coworkers20 concluded that one-third of patients who had consulted a sports medicine clinic for jumper’s knee were unable to return to sports for more than six months. In a study of 991 former elite male athletes, 20% reported that an injury was the main reason for stopping their athletic career.21 Most of the athletes were treated nonoperatively with NSAIDs and physical therapy, and, at the follow-up, 53% of the subjects in the jumper’s knee group reported having had to quit their sports career because of the knee problem.22
■ "The system represents an alternative treatment paradigm for the conservative management of tendinopathies, which lead to joint pain and osteoarthritis. JJ
Despite the prevalence of patellar tendinopathy and a variety of therapeutic approaches, including surgery, no definitive treatment option exists. Even after surgery, many patients are still plagued with reduced activity due to continued pain. In addition, it is not uncommon for an athlete to re-tear a cruciate ligament following successful surgery and long-term rehabilitation. During my time working with the US Ski Team, this was a frustration for the athletes as well as the medical staff.
Throughout my 26 years as the team chiropractic physician for the Utah Jazz, I have developed a model that defines the source of joint pain and the processes by which the body breaks down. It is based on the foundational work of Kendall and Kendall,23 Goodheart,24 and Beardall,25 and the growing field of mechanobiology26 and the pioneering work of Pleotz, Kummer, Benjamin, and Pauwels.26-27
The system represents an alternative treatment paradigm for the conservative management of tendinopathies, which lead to joint pain and osteoarthritis. It is a precision biomechanical and neurologically based system of assessment, diagnosis, and treatment for common injuries and conditions experienced by athletes and active people. It allows for the rapid determination of whether a problem requires surgery or whether the condition would be better served by conservative, less expensive, less invasive care. The purpose is to define areas of instability caused by muscles that have become inhibited due to traumas and overuse. Once these muscles are defined, the therapy allows the practitioner to reactivate the muscles that have become reflexively inhibited by the body’s proprioceptive system. The technique is entirely manual and combines several alternative approaches, such as clinical kinesiology, acupressure, proprioceptive neurology, and spinal manipulation. It allows for prediction of where injuries will occur and prevention by defining positions of instability. When an injury does occur, the healing process is accelerated, often getting athletes back into competition within minutes of sustaining an injury.
This process is based on the ideas that when a muscle is stressed beyond its capacity and the integrity of the muscle is exceeded, the small nerve endings in the tissue, called proprioceptors, trigger protective reflexes. These protective reflexes inhibit the muscle function by reducing the ability of the muscle to contract in a normal way when loaded. This is similar to a circuit breaker in an electrical circuit tripping when the system
* ^Following episodes of trauma, lesions at the enthesis may result in a wide range of symptoms. J J
is overloaded in order to protect the system. If this system fails, more severe damage occurs.
These protective reflexes include the muscle spindle cells located within the muscle body that monitor the intensity of the demand being placed on the muscle.
This allows for the activation of the appropriate number of muscle fibers needed to stabilize the demand being placed on it. This sensory system also allows the muscle fibers to determine where the body is in relationship to time and space and respond primarily to stretch. Next is the Golgi tendon organ located in the tendon of the muscle. If the muscle and tendon are stretched too rapidly, the tendon organ inhibits the muscle to protect it from injury and is essentially a “tension regulator.” Once the stress is removed from the muscle, it returns to normal function.
However, the body has a built-in “fail-safe” that, if the integrity of the aforementioned systems is exceeded, the proprioceptive centers located at the osteotendinous attachment inhibits the muscle much like a circuit breaker in an electrical circuit would. This osteotendinous attachment is called the “enthesis,” and according to many researchers is richly innervated. Palsey (1997) stated that “the tendioperiosteal attachment of the muscles (enthesis) appears to be an area that is especially susceptible to injury as a result of trauma. Because it is a structurally flawed, richly innervated, and metabolically active area, it may be the ‘weakest link’ and most reactive site in the musculoskeletal system. Following episodes of trauma, lesions at the enthesis may result in a wide range of symptoms. Treatment of these lesions may be crucial to the success of post-traumatic pain management.”28
I have defined this mechanism of inhibition as “enthesogenic neuro-proprioceptive muscle inhibition” (ENPMI).29 When a muscle is in an ENPMI state, it will still contract in passive range of motion, but if forced to contract under a load, it will give way in a weak response. This creates isolated muscle weaknesses leading to positions of instability. The body has to create stability any way it can, and so it restricts movement by antagonist muscles becoming hypertonic to restricted joint movement through that plane of motion. If the inhibited muscle is forced to support a load, pain occurs to protect. If the muscle is excessively or rapidly stressed, the muscle and/or connective tissue will tear. By defining the muscles that are not properly firing, future
injuries can be predicted and prevented. £ £
Pain is part of a sophisticated languaging system designed to protect the body.
It is a way for the body to tell us that we cannot stabilize a load through the plane of motion. When medication is used to relieve pain, it overrides an important protective system and joints break down prematurely. The human body is the most brilliantly orchestrated system on the planet, and pain is part of a sophisticated innate biological languaging system. When this language is
Repetitive muscle injuries lead to adhesions or scar tissue formation, which further restricts motion and causes more pain. J J
ignored or suppressed, the body is forced to adapt and compensate with other tissues. This increases the burden on those tissues that can become the next site of injury or symptoms. When the body is successful in adapting, the pain or symptoms may subside, lulling us into a false sense that everything is better. This leads to adaptive movement patterns, which lead to future injuries as the cycle continues.
Muscles must function as a synchronous whole to create
efficient motion. When muscle groups
like the quadriceps contract, they send nerve impulses to their antagonist muscles to inhibit them. The antagonists to the quadriceps are the hamstring muscles. When the hamstrings contract, the reverse process occurs. This is known as “reciprocal inhibition,” which allows us to walk or run in a smooth and coordinated manner.
When a muscle is in an ENPMI state, it loses its ability to neurologically inhibit antagonist muscles. As in the example of the quadriceps and hamstrings, if one of the quadriceps muscles is inhibited, the antagonist hamstring muscle is found to be facilitated. This leads to a hamstring muscle that is always contracted or tight through its inhibitory phase of motion. Therapies are used to intervene in this symptom by working to release the hamstring tension and increase flexibility. However, the tight hamstring is the body’s attempt to create stability when a muscle has become inhibited. It is protective in nature and so when we increase the range of motion of the tight muscle, we increase instability by removing the body’s defense system. If mobility is improved without increasing stability, injuries occur.
This chronically tight hamstring muscle is now susceptible to microtrauma and muscle fiber tearing. Repetitive muscle injuries lead to adhesions or scar tissue formation, which further restricts motion and causes more pain. This injury cycle continues with each new injury until the body can no longer adapt or compensate.
■ " Inflammation is designed to promote healing, and swelling is designed to help cushion and protect the joint in a healing cascade. 5 5
Muscles absorb most of the shock of weight bearing. When they become inhibited, they lose most of this shock-absorbing quality. When enough muscles in a given area are inhibited, connective tissues, such as ligaments, bursa, adipose tissue, and cartilage, are forced to take on a larger supportive role. These connective tissues are not designed to assume the extra burden. As a result, the body’s defense system activates pain centers, inflammation, and swelling to protect the joint. Pain acts to force a reduction in stress on the joint. Inflammation is designed to promote healing, and swelling is designed to help cushion and protect the joint in a healing cascade.
When the joint becomes inflamed or injured, a reaction known as arthrogenic muscle inhibition (AMI) occurs, causing further muscle inhibition and instability. AMI is a presynaptic, ongoing reflex inhibition of musculature surrounding a joint after distension or damage to that joint.30'35Arthrogenic muscle inhibition is a natural response designed to protect the joint from further damage. If a joint is irritated, injured, or inflamed, any muscle that attaches to or crosses over the joint will become inhibited. The presence of AMI retards rehabilitation despite complete muscle integrity. These defense systems are all part of nature’s genius. This reaction may provide an insight as to why manipulation of joints is so effective and is the foundation upon which the tenants of chiropractic can be partially defined.
As this process continues, connective tissues begin to break down leading to joint instability. Ligaments begin to stretch beyond normal limits and lose their tension regulatory function and ability to stabilize the joint. Although tendons and ligaments are often viewed as non-distensible, they do have the ability to stretch and recoil by approximately 6% of their original length without any obvious signs of damage.10 Once the tendon exceeds this limitation, damage begins to occur, leading to intense burning pain similar to nerve root pain. The muscles then go into a defensive splinting process leading to chronically tight regional muscles. Trigger points become active as the muscles naturally splint to protect the joint by limiting joint motion.
The body is continuing its attempt to stabilize a dysfunctional system. As time passes, joints begin to break down as arthritic changes occur and bone is more susceptible to stress
fractures. Eventually, the joint breaks down into complete degeneration. Ankylosing (self-fusing) and bony spurs are the last attempts by the body to stabilize the joint by restricting motion. All of this explains why a fifty-year-old patient can have an eighty-year-old knee requiring replacement.
^Ankylosing (self-fusing) and bony spurs are the last attempts by the body to stabilize the joint by restricting motion. All of this explains why a fifty-year-old patient can have an eighty-year-old knee requiring replacement. 5 J
Many therapies have been developed that can be effective at each of these stages of breakdown. Over the course of 50 years of cumulative clinical experience, new, effective, and conservative approaches to joint and muscle pain associated with sports chiropractic have been developed. This is accomplished without the use of drugs or surgery. Chiropractic manipulation is effective if the muscle inhibition is due to
neurogenic or arthrogenic muscle inhibition phenomenon. Active release technique (ART) offers an effective methodology of breaking adhesions created by multiple injuries to muscles and their fascia. Advanced Muscle Integration Technique® (AMIT) offers effective analysis, diagnosis, and corrective treatment in the most complex of conditions. It targets and corrects the effect of both AMI and ENPMI, and has been used successfully at the highest level of human athletic performance.
Using the discipline of chiropractic and integrating other healing disciplines, impressive results are created. Not only can we predict future injuries, we can correct acute injuries in a matter of minutes to have the athlete back in competition with pain-free, balanced, and stabilized function. Most importantly, human performance is taken to a new level.
SEE REFERENCES ON PAGE 52
□ Craig F. Buhler, D.C., F.I.C.C. graduate of Western States Chiropractic College in 1974-1978, and works in his clinic, Buhler Athletic Injuries & Human Performance. He also developed A.M.I.T.® (Advanced Muscle Integration Technique). An integrative biomechanical and neuro-proprioceptive approach to human performance analysis and treatment which accelerates healing, maximizes function and human performance. You can reach Dr. Buhler via telephone at 1-801-544-2355.