In this article, we have looked at some of the dynamics of the vertebral subluxation. The ligaments play a key role in the interrelationship of damaging force, muscular rebound, and proper correction. Joint stabilization is the key element in healing the musculoskeletal system.
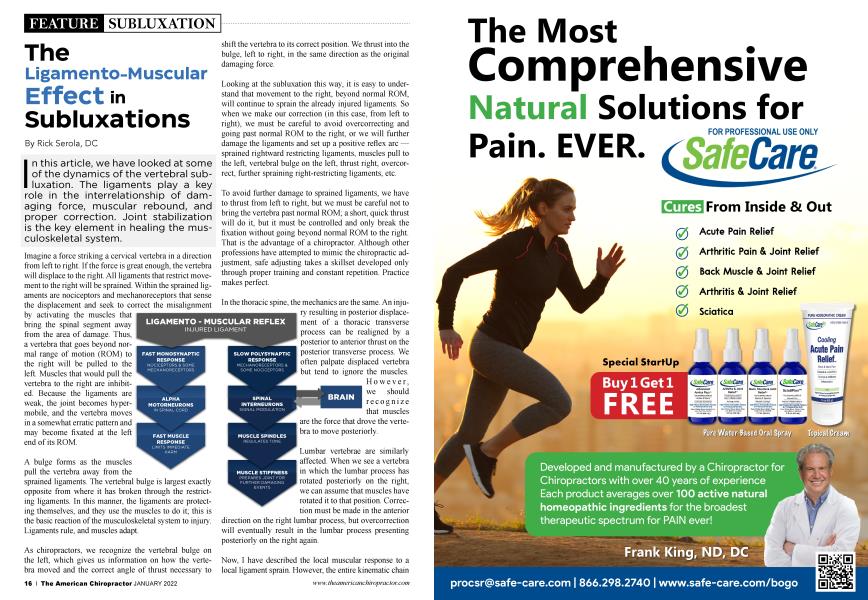
Imagine a force striking a cervical vertebra in a direction from left to right. If the force is great enough, the vertebra will displace to the right. All ligaments that restrict movement to the right will be sprained. Within the sprained ligaments are nociceptors and mechanoreceptors that sense the displacement and seek to correct the misalignment by activating the muscles that bring the spinal segment away from the area of damage. Thus, a vertebra that goes beyond normal range of motion (ROM) to the right will be pulled to the left. Muscles that would pull the vertebra to the right are inhibited. Because the ligaments are weak, the joint becomes hypermobile, and the vertebra moves in a somewhat erratic pattern and may become fixated at the left end of its ROM.
A bulge forms as the muscles pull the vertebra away from the sprained ligaments. The vertebral bulge is largest exactly opposite from where it has broken through the restricting ligaments. In this manner, the ligaments are protecting themselves, and they use the muscles to do it; this is the basic reaction of the musculoskeletal system to injury. Ligaments rule, and muscles adapt.
As chiropractors, we recognize the vertebral bulge on the left, which gives us information on how the vertebra moved and the correct angle of thrust necessary to shift the vertebra to its correct position. We thrust into the bulge, left to right, in the same direction as the original damaging force.
Looking at the subluxation this way, it is easy to understand that movement to the right, beyond normal ROM, will continue to sprain the already injured ligaments. So when we make our correction (in this case, from left to right), we must be careful to avoid overcorrecting and going past normal ROM to the right, or we will further damage the ligaments and set up a positive reflex arc — sprained rightward restricting ligaments, muscles pull to the left, vertebral bulge on the left, thrust right, overcorrect, further spraining right-restricting ligaments, etc.
To avoid further damage to sprained ligaments, we have to thrust from left to right, but we must be careful not to bring the vertebra past normal ROM; a short, quick thrust will do it, but it must be controlled and only break the fixation without going beyond normal ROM to the right. That is the advantage of a chiropractor. Although other professions have attempted to mimic the chiropractic adjustment, safe adjusting takes a skillset developed only through proper training and constant repetition. Practice makes perfect.
In the thoracic spine, the mechanics are the same. An injury resulting in posterior displacement of a thoracic transverse process can be realigned by a posterior to anterior thrust on the posterior transverse process. We often palpate displaced vertebra but tend to ignore the muscles.
However, we should recognize that muscles are the force that drove the vertebra to move posteriorly.
Lumbar vertebrae are similarly affected. When we see a vertebra in which the lumbar process has rotated posteriorly on the right, we can assume that muscles have rotated it to that position. Correction must be made in the anterior direction on the right lumbar process, but overcorrection will eventually result in the lumbar process presenting posteriorly on the right again.
Now, I have described the local muscular response to a local ligament sprain. However, the entire kinematic chain may act in a series for a core injury at the sacroiliac joint (SIJ). By pulling the sacrum or ilium into a corrective pattern, the other ends of the muscles will affect the spine and extremities, inducing torque that alters vertebral alignment throughout the body. A local vertebral misalignment may actually be part of a more global disturbance.
Hilton’s Law states that all muscles that attach to bones that make up a joint are innervated and, therefore, regulated by the nerves within the joint. The joint itself consists mainly of the ligaments; the nerves sit within the ligaments.
When the SIJ is subluxated, the ligaments become sprained, inducing the sacrum and ilium to misalign in the direction away from the sprained ligaments. Thus, we have to look at what direction the sacrum and ilium move, which ligaments restrict that movement, and which muscles pull those bones in the opposite direction. The first one is easy. The sacrum and ilium move in nutation and counternutation; they do not move in a medial to lateral direction.
Nutation is a screw-like movement involving all three planes as the sacrum moves anterior, inferior, and rotates to the opposite side, relative to the ilium. Nutation is the movement toward the bottom point of shock absorption where weight transfers between the sacrum and ilium. Conversely, counternutation is the movement toward the upper point in rebound, where relatively little, if any, weight transfers between the sacrum and ilium.
For this reason, the ligaments that restrict nutation undergo the most stress; they restrict weight transfer at the core of our pelvis — the sacroiliac joint. These nutation-limiting ligaments comprise the bulk of SIJ ligaments and include the interosseous, sacrospinous, sacrotuberous, etc. The muscles that pull the joint away from injury are those that induce counternutation (e.g., the piriformis, quadratus lumborum, iliopsoas, hip flexors, etc.), which comprise the bulk of our musculature.
Just as we will see the cervical vertebrae bulge on the left when the damaging force comes from the left, we will see the sacral misalignment occur in counternutation when the damaging force induces nutation. In an attempt to remove stress from ligaments within the joint, the muscles that would stabilize the joint are activated, and the muscles that would destabilize the joint are inhibited. The structure moves away from the sprained ligaments.
Because an SIJ injury is usually in nutation, we see the patient in a pattern of counternutation on the side of injury; simply put, the sacrum is posterior, and the ilium is relatively anterior. As with other vertebrae, the correction is to move the pelvis away from the compensated pattern toward nutation on the side of injury, which means adjusting the anterior side of the pelvis backward and the posterior side of the pelvis forward. Ideally, the patient will end up with a balanced pelvis in which the sacrum and ilium on both sides are evenly aligned.
As with other joints, do not go past normal ROM during treatment, or you will re-sprain the damaged ligaments. Because many doctors and therapists are not aware of the consequences of the ligamento-muscular reflex, they may continue adjusting or stretching repeatedly, inducing a destructive cycle. The more forceful the thrust or stretch, the more damage to the ligaments. Eventually, the joint becomes hypermobile, which complicates recovery.
One way to look at it is that the damaging force has separated the joint, and the muscles contract to pull the joint back together. So, when we stretch the tight muscles, we are actually pulling the joint apart. The same thing happens when we strengthen the inhibited muscles. Both sets of muscles — tight and lax — don’t pump properly, which causes insufficient circulation. Reduced circulation results in reduced oxygen and a build-up of cellular waste, which are common mechanisms that cause pain in the musculoskeletal system.
So, why does it feel so good? By increasing circulation, we are temporarily increasing oxygenation and washing out the metabolic toxins. Here is another important point; it takes time — maybe days, weeks, or even months for active people — for the toxins to build up in the muscles again to the point where they can cause pain. So, if we do our stretching or strengthening often enough, we don’t have time to build up the toxins that cause pain, so we mistakenly think the treatment is beneficial. In our minds, time dissipates the connection between cause and effect.
Eventually, the patient feels better and has greater mobility. It seems like all is good, but actually, the joint is worse off after treatments. In any case, we all know that pain and misalignment will probably return, so the patient is given exercises or stretches to help with recurring pain. Unfortunately, by doing this, they instill a destructive positive feedback cycle that, over time, perpetuates a chronic dysfunction that may spread throughout the body. The sprained ligaments will continually be re-sprained, and the muscular imbalance and pain become chronic — shortterm success yields to long-term degeneration.
The only way to treat the patient successfully is to stabilize the joint with something that prevents excess ROM and provides appropriate compression, whether it is with a collar, brace, belt, or procedure. By stabilization, it is meant that the joint remains within its normal ROM; any excess movement will reinjure the ligaments and delay or prevent healing. When the joint is stabilized, most ligaments will heal.
However, because of the dynamics of the sacroiliac joint, healing is more complicated. The interosseous ligaments do not tear in the middle; they pull away from the joint surfaces. Healing involves aligning and compressing the syndesmoses of the SIJ in such a manner that allows the ligaments to reintegrate into the joint surfaces.
Fortunately, Dr. DeJarnette developed supine pelvic blocking (category 2) specifically for this purpose. While a correctly made sacroiliac belt can stabilize the SIJ while a patient wears it, category 2 is the only procedure that can stabilize the SIJ on a permanent basis.
Rick Serola, DC graduated Summa Cum Laude from Palmer College of Chiropractic in 1983, as a member of the Chiropractic Honor Society. He is the founder and Co-CEO of Serola Biomechanics, Inc., which manufactures orthopedic solutions, and is the result more than 30 years of clinical research into biomechanics. Through his research, he also developed a theory on biomechanics, The Musculoskeletal Integration Theory, which is the only model that ties the musculoskeletal system into a functioning whole. He has won the State Line World Trade Association's Exporter of the Year Award in 2009. 2019 Mid-America Trade Summit's Award for Exporting Excellence, 2019 Illinois Governor's Export Award, and 2020 Presidential "E" Award for Exporting Excellence.