Some of your patients may have commented that one or more of their joints feel like they are going to “go out of place” or “give out.” Many of you know the feeling: if you move the wrong way, your knee feels like it’s going to collapse, or your low back is going to complain; or if you move your shoulder the wrong way, you’ll feel a “pinch.” All of these symptoms are due to one of the most common issues we are confronted with in daily practice—whether we realize it or not—unstable joints. It is important to note that articular instability can accelerate pathophysiology in the soft tissues (cartilage, ligaments, tendons) and the osseous components of the joint, leading to wear-and-tear and ultimate failure of these structures. 2,3
Most references to unstable joints attribute the problem to weaknesses, partial tears or complete tears of ligaments. Patients are initially provided with one of many forms of external stabilizing devices or multicolored tape. If that doesn’t work, they are injected with several types of sclerosants (prolotherapy), and when all of those eventually fail, surgery is often performed to correct or replace the damaged ligaments. However, several studies have revealed that the diagnosis of a “torn” ligament does not often agree with the findings of the surgeon. In one study the results of MRIs, and the actual surgical finding of a complete cruciate ligament tear, agreed no more than 67% of the time, suggesting that these imaging techniques should not be relied on. 1
When we consider that almost every activity involves complex and constantly changing biomechanical relationships within the musculoskeletal system, including posture, weight-bearing, gait, athletic performance and general activities of daily living, it seems logical that some form of dynamic stabilization would be required. I speculated that a key missing element in understanding the mechanism of stability is a neuromuscular component, which would account for the moment-to-moment stability requirements for complex biomechanical function. Several studies have confirmed that this is indeed the case. 2,3
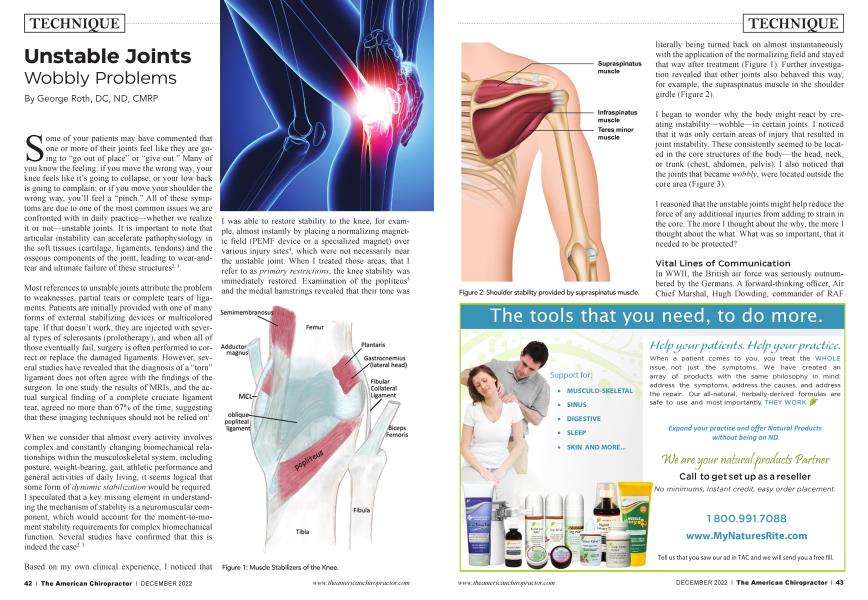
Based on my own clinical experience, I noticed that I was able to restore stability to the knee, for example, almost instantly by placing a normalizing magnetic field (PEMF device or a specialized magnet) over various injury sites4, which were not necessarily near the unstable joint. When I treated those areas, that I refer to as primary restrictions, the knee stability was immediately restored. Examination of the popliteus3 and the medial hamstrings revealed that their tone was literally being turned back on almost instantaneously with the application of the normalizing field and stayed that way after treatment (Figure 1). Further investigation revealed that other joints also behaved this way, for example, the supraspinatus muscle in the shoulder girdle (Figure 2).
I began to wonder why the body might react by creating instability—wobble—in certain joints. I noticed that it was only certain areas of injury that resulted in joint instability. These consistently seemed to be located in the core structures of the body—the head, neck, or trunk (chest, abdomen, pelvis). I also noticed that the joints that became wobbly, were located outside the core area (Figure 3).
I reasoned that the unstable joints might help reduce the force of any additional injuries from adding to strain in the core. The more I thought about the why, the more I thought about the what. What was so important, that it needed to be protected?
Vital Lines of Communication
In WWII, the British air force was seriously outnumbered by the Germans. A forward-thinking officer, Air Chief Marshal, Hugh Dowding, commander of RAF Fighter Command developed a coordinated communication network to link all of the airfields in southern England. This involved an elaborate and efficient system of telephone lines, heavily protected from damage by being buried very deeply underground, and protected by tons of concrete. Dowding foresaw the need to create and protect these vital lines of communication fully 5 years before the start of WWII, based on his view of the potential threat of the rise of Nazism. His foresight likely saved Britain from invasion.
I found this story intriguing, and it reminded me of another vital communication system, without which, the human body cannot survive—the spinal cord. The spinal cord must be protected from injury at all costs. In fact, the vertebral column, through which it passes, is so perfectly designed that none of the complex movements it is capable of performing ever causes the least amount of pressure on its precious contents. One of the ways it accomplishes this biological and engineering marvel is via the intricate paraspinal muscles (multffidi, rotatores, etc.), which are richly supplied with sensory and motor neurons that allow them to act as powerful and coordinated neuromuscular ligaments. This allows the nervous system to continuously adapt to changes in posture and movement, while protecting the integrity of the spinal cord. This holds true except for one notable exception—the low back.
Low Back Instability
The lower lumbar spine is famous for “going out,” “slipping,” or becoming “strained.” I noticed that the lower lumbar vertebrae behaved in the same way as the knee and the shoulder. The paraspinal muscles in this part of the spine became noticeably hypotonic, and the movement between the vertebrae, became lax. When I applied a normalizing magnetic field to injured core structures, the muscle tone5 and joint stability immediately improved.
This makes sense when we recall that one of the overriding priorities for survival is to maintain the integrity of one of the main lines of communication—the spinal cord. The spinal cord itself ends in the upper to middle part of the lumbar spine (L2, 3), whereas the lower lumbar spine contains individual nerve bundles (cauda equina), which are less vulnerable to damage from vertebral dysfunction (Figure 4).
Thus, the lower lumbar spine appears to be sacrificed to protect the more important portions of the spinal column surrounding the spinal cord. This may result in pain and limited motion, but would not likely lead to paralysis, the way an injury to other portions of the spine might. A similar mechanism appears to affect the muscles of the hip, knee, shoulder, ankle, and wrist.
Turning Joint Stability Back On... Like Flipping a Switch!
Remarkably, treatment of primary restrictions in the core structures, appears to consistently and immediately restore stability in the so-called sacrificial joints. What might account for this response? Once I recognized how certain so-called stabilizing muscles were involved in mediating the stability of these joints, I speculated that this must represent some type of neuromuscular reflex response.
It is my current theory, which I refer to as the Articular Stability Reflex (ASR), that there may be a feedback mechanism, mediated via spinal reflexes or mechanical-electro-chemical signals generated within the extracellular matrix (ECM)6. These systems may be able to monitor potentially threatening injuries and respond by triggering inhibitory or excitatory efferent neurons at the spinal level. Whatever the mechanism may be, it appears to allow the body to rapidly modulate stability of the peripheral, appendicular joints, including—notably—the lower lumbar spine.
In conclusion, many painful conditions of the knee, shoulder, low back, and several other areas, appear to be due to instability in these joints. Many practitioners, using this approach, have confirmed that joint stability is often restored almost immediately after the underlying primary restrictions are addressed7. In this way, they have been able to help many conditions associated with joint instability, resulting in significant clinical improvement and support for tissue repair. Further research is required to assess the effectiveness of this approach on the possible reversal or prevention of degenerative changes associated with these joints.
Dr. George Roth, BSc, DC, ND, CMRP is recognized as an authority and pioneer in the field of physical medicine. He is the developer of Matrix Repatterning, a breakthrough treatment system that is recognized worldwide. He is the author of The Matrix Repatterning Program for Pain Relief and his contribution to the treatment of concussion and traumatic brain injury has been acknowledged by Dr. Norman Doidge in his best-selling book, The Brain's Way of Healing.
References:
1. Tsai, K, et al. (2004), “Magnetic resonance imaging of anterior cruciate ligament, ” BMC Musculoskelet Disord. 2004; 5: 21, doi: 10. 1186/1471-2474-5-21
2. Structural joint changes, malalignment, and laxity in osteoarthritis of the knee, M. van der Esch, M. Steultjens, H. Wieringa, H. Dinant, J. Dekker, Scandinavian Journal of Rheumatology, 2005, Vol. 34, No. 4, Pages 298-301
3. The proximal attachments of the popliteus muscle: a quantitative study and clinical significance. V. Feipel, M.L. Simonnet, M. Rooze. Surg. Radiol Anat. (2003) 25: 58-63.
4. MacGuintie LA, Streaming and piezoelectric potentials in connective tissues. In: Blank M (ed.) Electromagnetic fields: biological interactions and mechanisms. Advances in Chemistry Series 250. American Chemical Society, Washington DC, ch. 8, pp 125-142, 1995.
5. A. Asher, Multifidus Muscle: Its Function and Link to Back Pain: Its Function and Link to Back Pain, A muscle that he