A Chiropractic Approach to Shoulder Pain
REHAB
Kevin M. Wong
DC
Kevin M. Wong, DC, is a graduate of the University of California, Davis, and a 1996 graduate of Palmer College of Chiropractic West. He has been in practice for over 26 years and is the owner of Orinda Chiropractic & Laser Center in Orinda, California. As a member of Foot Levelers ’ Speakers Bureau since 2004, Dr. Wong travels the country speaking on extremity and spinal adjusting.
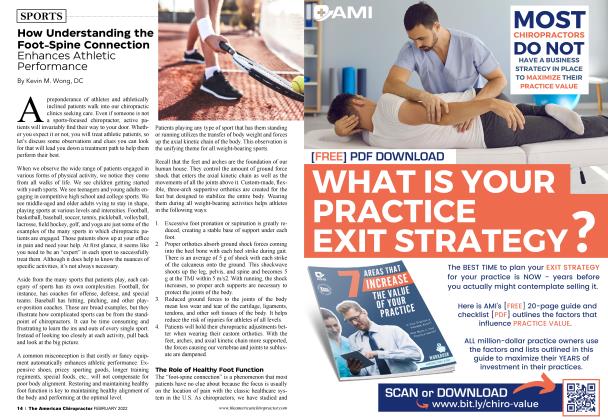
Much of the general patient population does not understand that chiropractors treat the extremities of the body. Chiropractors have long been labeled as “back and neck doctors.” Although those are appropriate areas of the body with which to be associated, chiropractors are well qualified to assess and treat all extremities of the body. With extremity pain being such a common presentation, proficiency in identifying and treating it is important.
Shoulder pain is one of the most frequent complaints from patients presenting to a chiropractic clinic. Academically speaking, we have been taught that the shoulder may be the location of referred pain originating from the neck or upper back. While this can be tine, more often, we observe that the shoulder is the primary problem, and its instability can negatively influence the neck, upper back, and ribs.
Shoulder Pain Is Not Rare!
Shoulder pain is the third most common musculoskeletal complaint, and several cost-of-illness studies suggest it is a very significant malady (Hodgetts et al., 2021). Common diagnoses can be broken down into categories like intra-articular, anterior shoulder, and subacromial. Despite surgery rates increasing in some areas, multiple systematic reviews suggest there is no difference in pain and disability outcomes between surgical interventions and conservative approaches.
The joints of the shoulder are frequently misaligned, necessitating attention for stability.
Several studies have revealed that only 50% of all new cases of shoulder pain completely recover after six months and 60% after 12 months.
A systematic review of the global prevalence and incidence of shoulder pain looked at 61 studies reporting data from high, middle, and low-income countries (Lucas et al., 2022). It found that a significant proportion of the population across the world would experience shoulder pain daily, yearly, and throughout their lifetime.
An epidemiologic survey of shoulder pain in chiropractic practice found the prevalence of shoulder pain symptoms, as reported by the practitioners, was 12% of the total weekly patients, with the major cause of symptoms related to overuse (32%) (Pribicevic et al., 2009). The most prevalent working diagnosis of shoulder pain was shoulder impingement syndrome (13%), followed by impingement syndrome with rotator cuff tendinosis (17%), impingement syndrome without rotator cuff tendinosis (14%), and chiropractic shoulder subluxation (12%).
Chiropractors and manual therapists have understood for years that no matter what shoulder ailment is occurring, the unifying theme is that the joints of the shoulder are all out of alignment. These misalignment patterns are frequently observed and must be addressed for any type of stability to be obtained.
The Relationship of the Shoulders to the C/T Spine
The shoulders have a profound influence on occiput, neck, upper back, and shoulder stability. Patients don’t understand this relationship; interestingly, many healthcare providers don’t either. Frequently, patients are observed describing pain beginning in the occiput and moving down the neck, upper back, and mid-back on the ipsilateral side. This phenomenon is seen in many patient presentations and is the first step in recognizing a pattern that can be used for treatment later.
Examination Sets up Chiropractic Care
Use visual observations of the shoulder girdle to clue you in to the involved areas. Orthopedic testing helps rule in/out and identify any common shoulder maladies. Impingement is one of the main causes of inflammation, and pain in the shoulder is a secondary effect of a variety of conditions (bursitis, tendonitis, frozen shoulder, and partial or complete tears of the rotator cuff or labrum).
Special imaging may be indicated for more clarification. It’s also likely that by the time the patient seeks chiropractic care, they have already been to a number of other healthcare practitioners, and they previously had imaging. The radiology report and diagnosis from a previous medical provider may provide more information to diagnose the patient.
Evaluate the Entire Thoracic Spine and Shoulder Complex
Remember that the shoulder is more than just the ball-and-socket joint. Look at the glenohumeral, acromioclavicular, sternoclavicular, and scapulothoracic joints, thoracic spine, and 12 sets of ribs in the back and front.
Visual comparisons of the left and right sides of the body, along with observing the shoulder, scapular, rib, and thoracic range of motion (ROM), are additional effective tools for identifying problem areas. Palpate these joints to really sharpen the picture of what is involved and in which direction the bones have subluxated.
Palpating the musculature around the shoulder region helps identify the side of shoulder involvement and the directions the bones have subluxated. Biceps, pectoralis, anterior/middle/posterior deltoid, upper/middle/lower trapezius, levator scapulae, and the four rotator cuff muscles can be hypertonic because the shoulder joints are out of alignment.
Treatment
Identify the common clinical subluxation patterns and how to adjust them
It is very common for all of the patient’s shoulder joints to be involved in being out of alignment. We can observe a typical shoulder region subluxation pattern that occurs in a majority of patients. The pattern is listed below, and for simplicity, the directions in which to correct the alignment of the bones are also provided.
• GH jt: Humeral head moves anterior/inferior
(Adjust humeral head posterior/ superior)
• AC jt: Distal clavicle moves superior
(Adjust distal clavicle superior to inferior)
• SC jt: Proximal clavicle moves superior/anterior/medial (Adjust proximal clavicle superior/anterior/ medial)
• Scapulothoracic: Scapula subluxates in upward rotation (Adjust into downward rotation)
• Ribs: Rib heads in front and back subluxate superior most of the time. (Adjust inferior on rib head either at the sternum in the front or costotransverse joint in the back)
Thoracic Spine
Observe vertebral rotational patterns along with rib subluxations and adjust accordingly.
a. Shoulder adjustments are effective
In one particular study, a systematic review of manual and manipulative therapy for common shoulder pain and disorders was conducted (Brantingham et al., 2011). There is fair evidence for the treatment of a variety of common rotator cuff disorders, shoulder disorders, adhesive capsulitis, and soft tissue disorders using manipulative therapy on the shoulder, shoulder girdle, or the full kinetic chain combined with or without exercise and multimodal therapy.
The typical subluxation or misalignment patterns of the shoulder are typical for most patients. Now, you (the practitioner) get to decide how you will correct the bone. A variety of adjustments utilizing manual, drop-table, and handheld instruments will do the job. In this region of the body, having command of different adjusting methods allows you to treat a variety of patients.
The trick with the shoulder is to drop the humeral head away from the acromion to decompress the region. I mostly utilize a drop table to align the shoulders, but the classic manual adjustments, using the spring-loaded instruments, or employing plug-in adjusting tools works well also. Remember, gauge where your patient is and what they can handle based on their symptom presentation and diagnosis. It’s usually prudent to go lighter in force and give the body time to react and begin to heal.
b. Support
1. Elastic sports tape
Taping can be utilized to support the AC, SC, GH, rib heads, and vertically on both sides of the thoracic spine. Tape can even be applied around the sides and anteriorly along the ribs for support too. Tape can be utilized to hold joints in place after you have adjusted them. Tape is easy to apply, comfortable to wear, and patients can learn to tape themselves.
2. Chiropractic-approved pillow
The pillow you sell in your office should be supportive enough for your patients to sleep on their side or back with their heads properly supported. Having patients bring their pillows in for you to evaluate is effective because you can determine if their current pillow works or if they need to replace it.
3. Scan or cast for custom three-arch, flexible foot orthotics
The feet are the foundation of the body. Overpronation or flattening of the three arches of the feet will cause negative biomechanical stress up the kinetic chain to the thoracic spine, shoulders, and ribs. If you are going to do the work on the top portion of the body, then don’t forget to do the work on the bottom part of the body (the feet) too. Almost everyone has some degree of overpronation and would benefit from custom stabilization, which also protects your adjustments and boosts the effectiveness of your care.
Rehabilitation
The presence of major injuries like rotator cuff tears, labium tears, or frozen shoulder will obviously impact the initial stages of what can be accomplished with rehab. In general, many patients we see in our chiropractic clinics have milder issues that really boil down to the shoulder joints being misaligned. Once they are adjusted and back in alignment, basic rehab protocols can be employed.
Opting for simple rehab might be the easiest way to go. Stretching of affected muscles, ROM exercises, and introducing elastic tubing/band exercises are all low-tech but extremely effective. Elastic tubing/bands are affordable, portable, and allow for resistive exercises to be performed in specific directions and varying speeds to help stabilize and strengthen the shoulder girdle musculature.
Chiropractic care can have a powerful influence on helping patients with both acute and chronic shoulder pain. Considering the vast number of patients who suffer from shoulder problems, this is an opportunity for chiropractors to position themselves effectively to help their patients heal naturally.
References:
1. Hodgetts, C. & Walker, B. (2021). Epidemiology, common diagnoses, treatments and prognosis of shoulder pain: A narrative review. International Journal of Osteopathic Medicine, 42, 11-19. https://doi. ore/10.1016/i.iiosm.2021.10.006 (https://www.sciencedirect.com/ science/article/pii/S 1746068921000821)
2. Lucas, J., van Doom, P., Hegedus, E., Lewis, J., & van der Windt, D. (2022). A systematic review of the global prevalence and incidence of shoulder pain. BMC Musculoskelet Disord, 23, 1073. https://doi. org/10.34961/researchrepositorv-ul. 228 8596 l.vl
3. Pribicevic, M., Pollard, EL, & Bonello, R. (2009). An epidemiologic survey of shoulder pain in chiropractic practice in Australia. Journal of Manipulative and Physiological Therapeutics, 32(2), 107-117. https://doi.org/!0.1016/i.impt...
4. Brantingham, J. W., Cassa, T. K.. Bonnefin, D., Jensen, M., Globe, G., Hicks, M., & Korporaal, C. (2011). Manipulative therapy for shoulder pain and disorders: expansion of a systematic review. Journal of Manipulative and Physiological Therapeutics, 34(5), 314-346. https:// doi.ordl0.m6/\.imnt.2011.04.002