The Science of Low Back Pain
TECHNIQUE
Providing Insights for Better Solutions
Dr. George B. Roth
BSc, DC, ND, CMRP
BACK PAIN IS THE SINGLE leading cause of disability, preventing many people from engaging in work and other daily activities.1 It is one of the most common reasons for missed work, with 50% of the working population experiencing symptoms each year.2 It is estimated that up to 80% of the population will experience low back pain at some time in their lives.3
Most people with low back pain recover, but reoccurrence is common, and for a small percentage of people, the condition will become chronic and disabling.4 Low back pain in the United States alone results in approximately $50 billion in healthcare costs each year. Add in lost wages and decreased productivity, and that figure easily rises to more than $100 billion.5
Practitioners from a variety of fields have tried every conceivable method to alleviate the pain and discomfort of this often-debilitating condition. The challenge, of course, is that most of the approaches have failed to provide long-term solutions. If you have found this condition to be challenging in certain cases, I encourage you to continue reading.
In this article, I will present some breakthrough concepts that may help explain some of the underlying causes of low back pain, and, by extension, many other painful biomechanical disorders. I hope to shed light on why some of the approaches currently in use may be missing some important underlying elements, namely some of the latest scientific evidence of how the body is constructed at the cellular and molecular levels. I believe a better understanding of how the body responds to injury at the most fundamental level may provide us with the insights necessary to provide real and lasting solutions.
The Physics of Injury
Walking the earth on two legs has provided humans with tremendous advantages, including freeing the upper extremities to be able to manipulate the environment (gather food, wield tools and weapons), presenting a higher profile to deter predators, and being able to survey our surroundings for potential threats and opportunities. However, one of the main trade-offs is that the upright, bipedal posture has made us more vulnerable to the laws of physics, namely gravity, inertia, and momentum.
As a result of this vulnerability, we begin the assault on our bodies at a fairly young age. From the moment we set forth on two toddling legs, this often takes the form of slipping and falling on the ground or the stairs, bumping into furniture, tripping over toys, and bumping our heads on cupboards, door frames, and our siblings. As we get older, we tend to engage in activities that put us at further risk for injury, such as high-speed and contact sports, motor vehicle collisions, etc.
The Importance of Bone Size
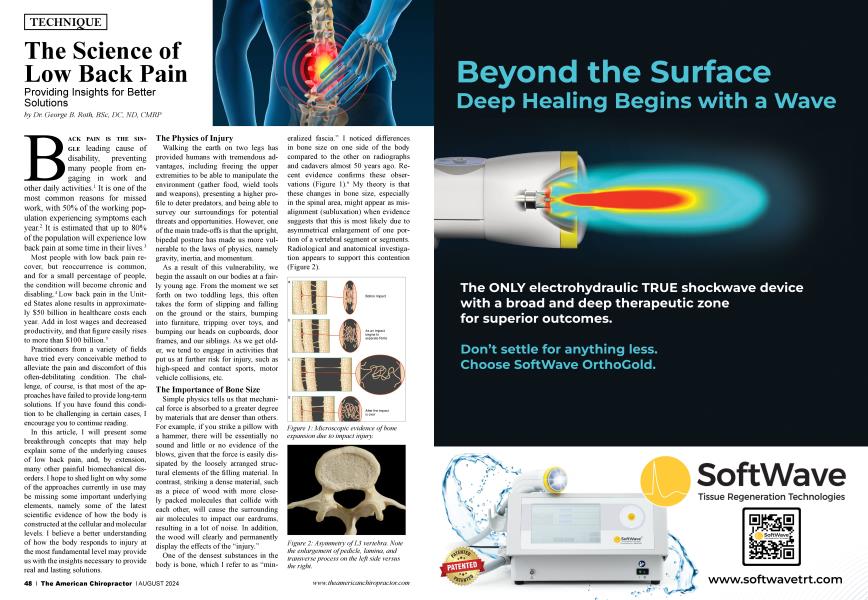
Simple physics tells us that mechanical force is absorbed to a greater degree by materials that are denser than others. For example, if you strike a pillow with a hammer, there will be essentially no sound and little or no evidence of the blows, given that the force is easily dissipated by the loosely arranged structural elements of the filling material. In contrast, striking a dense material, such as a piece of wood with more closely packed molecules that collide with each other, will cause the surrounding air molecules to impact our eardrums, resulting in a lot of noise. In addition, the wood will clearly and permanently display the effects of the “injury.”
One of the densest substances in the body is bone, which I refer to as “mineralized fascia.” I noticed differences in bone size on one side of the body compared to the other on radiographs and cadavers almost 50 years ago. Recent evidence confirms these observations (Figure I).6 My theory is that these changes in bone size, especially in the spinal area, might appear as misalignment (subluxation) when evidence suggests that this is most likely due to asymmetrical enlargement of one portion of a vertebral segment or segments. Radiological and anatomical investigation appears to support this contention (Figure 2).
As you will read in the next section, these local areas of bone expansion create sources of restriction that result in strain and pain in other areas of the body. Thus, the actual source of symptoms may remain elusive. Fortunately, I discovered a method to detect these deeper, underlying injuries within bone caused by changes in their bioelectric properties7 8
The Hip Bone’s Connected to... Everything!
It is now known that body tissues form a continuous framework, which we refer to as the “tensegrity matrix.” The internal framework of each cell (cytoskeleton) is supported by proteins, such as actin and tubulin, while the extracellular matrix (ECM), which interconnects every cell to its neighbors, is composed of various proteins and polysaccharide filaments. These elements have specific structural, mechanical, and electronic properties at the heart of how the mechanical influence of an injury affects the body. The application of the concept of tensegrity to biological systems, (also referred to as Biotensegrity), elaborated by Stephen Levin, MD,9 and Donald Ingber, MD, PhD,10 among others,11 holds that body tissues are composed of an interconnected framework, which provides a balance between stability and mobility.
Therefore, a source of restriction because of an injury in one part of the body, which we refer to as a primary restriction (localized area of tissue tension associated with pathophysiological and electromechanical alterations of cellular and molecular elements), is instantaneously transmitted to surrounding structures. That explains how patterns of tension arising from one primary restriction create tension and aberrant motion in structures throughout the entire body,12 which results in biomechanical dysfunction and increased strain on pain-sensitive structures, such as fascia, muscles, and joints. The resulting strain patterns are illustrated in Figure 3.
The primary restriction is often painless after the acute phase and only becomes painful upon direct stimulation (local tenderness similar to trigger points). This structural model explains many of the observed phenomena related to body support, movement, and response to stress and trauma and the effects of therapeutic interventions.
The Role of Stability
In the mid-1990s, I accidentally discovered a mechanism that appears to explain how the loss of stability in certain joints may contribute to the development of pain and articular degeneration. Muscles provide dynamic stabilization, such as the popliteus (knee), supraspinatus (shoulder), gluteus medius (hip), and multifidus, rotatores, intertransversarii, and interspinales for the lower lumbar spine (see Figure 4),13-15 and they literally turn off in response to certain injuries.
I speculated that this mechanism, which I refer to as the “articular stability reflex” (ASR), would have to mitigate the transfer of additional strain to core structures, including the spinal cord, by creating a “wobble zone” in the peripheral joints, which I refer to as “sacrificial joints.” It is important to note that the spinal cord is not present in the lower lumbar spine, which might explain why it is also sacrificed, so to speak.
Exercise programs aimed at improving “core strength” have been promoted to counteract this response, but I contend that it is impossible to strengthen these particular muscles because they are essentially denervated, i.e., turned off. It would be like repeatedly changing the light bulb in a lamp that is not plugged into an outlet in an attempt to make it work. The resultant instability may play a role in the degeneration of those structures by increasing mechanical stress on articular cartilage, menisci, subtending bone, and the intervertebral disc, in the case of the lower lumbar spine.
Our experience has demonstrated that treatment of the underlying structures that initiate the ASR tend to reestablish normal tone and function of the stabilizing muscles, which restores joint stability, much like turning on a light switch. This, along with the methods we have developed to restore normal bone size and structure, appears to be able to resolve many acute and chronic cases of low back pain.16
Summary
Our assumptions about the causes of many structural conditions, including low back pain, may need to be revisited in light of scientific discoveries related to the underlying structure of the body and how it responds to injury at the most fundamental level. Our understanding of the consequences of physical trauma in the form of impact or strain has evolved significantly in the past 50 years, and it is essential that we adapt our clinical interventions to incorporate these discoveries and provide our patients with the lasting and profound solutions now within our grasp.
Dr. Roth is a graduate of the University of Toronto, Canadian Memorial Chiropractic College, and the Ontario College of Naturopathic Medicine. He a|S0 studied osteopathic medicine at Doctors’ Hospital North, Columbus, Ohio. He developed Matrix Repatterning and is the director of education at the Matrix Institute in Toronto. Dr. Roth has presented seminars at numerous hospitaland university based symposia throughout North America. He is the coauthor with Kerry D’Ambrogio, PT, of Positional Release Therapy (Elsevier, 1997) and the author of The Matrix Repatterning Program for Pain Relief (New Harbinger, 2005). His work is also featured in The Brain’s Way of Healing by Dr. Norman Doidge (Penguin, 2015). For more information, visit www.matrixforpractitioners.com.
References
1. Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, Williams G, Smith E, Vos T, Barendregt J, Murray C, Burstein R, Buchbinder R. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014 Jun;73(6):968-74. doi: 10.1136/annrheumdis-2013-204428. Epub 2014 Mar 24. PMID: 24665116.
2. Vallfors B. Acute, subacute and chronic low back pain: clinical symptoms, absenteeism and working environment. Scand J Rehabil Med Suppl. 1985;11:1-98. PMID: 3161177.
3. Rubin DI. Epidemiology and risk factors for spine pain. Neurol Clin. 2007 May;25(2):353-71. doi: 10.1016/j. ncl.2007.01.004. PMID: 17445733.
4. Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J, Pransky G, Sieper J, Smeets RJ, Underwood M. Lancet low back pain series working group: what low back pain is and why we need to pay attention. Lancet. 2018 Jun 9;391(10137):2356-2367. doi: 10.1016/S01406736(18)30480-X. Epub 2018 Mar 21. PMID: 29573870.
5. Katz JN. Lumbar disc disorders and low-back pain: socioeconomic factors and consequences. J Bone Joint Surg Am. 2006 Apr;88 Suppl 2:21-4. doi: 10.2106/JBJS.E.01273. PMID: 16595438.
6. Fantner GE, Hassenkam T, Kindt JH, Weaver JC, Birkedal H, Pechenik L, Cutroni JA, Cidade GA, Stucky GD, Morse DE, Hansma PK. Sacrificial bonds and hidden length dissipate energy as mineralized fibrils separate during bone fracture. Nat Mater. 2005 Aug;4(8):612-6. doi: 10.1038/nmatl428. Epub 2005 Jul 17. PMID: 16025123.
7. Chakkalakal DA. Mechanoelectric transduction in bone. J Mater Res. 1989;4(4), 1034-1046. doi:10.1557/JMR.1989.1034
8. Heng BC, Bai Y, Li X, Meng Y, Lu Y, Zhang X, Deng X. The bioelectrical properties of bone tissue. Animal Model Exp Med. 2023 Apr;6(2): 120-130. doi: 10.1002/ame2.12300. Epub 2023 Mar 1. PMID: 36856186; PMCID: PMC10158952.1.
9. Levin, SM. The importance of soft tissues for structural support of the body. Spine: State of the Art Reviews. 1995 May;9(2). Available from: https://www.researchgate.net/publication/281364767_The_importance_of_soft_ tissues_for_structural_support_of_the_body
10. Ingber DE. The architecture of life. Sci Am. 1998 Jan;278(l):48-57. doi: 10.1038/scientificamericanOl98-48. PMID: 11536845.
11. 11. Pischinger, A. The Extracellular Matrix and Ground Regulation: Basis for a Holistic Biological Medicine. North Atlantic Books, Berkley; 2007. Available from: https:// books.google.com/books?id=Cc2AkgEACAAJ
12. Mannion AF. Fibre type characteristics and function of the human paraspinal muscles: normal values and changes in association with low back pain. J Electromyogr Kinesiol. 1999 Dec;9(6):363-77. doi: 10.1016/s 10506411(99)00010-3. PMID: 10597049.
13. Beazell JR, Mullins M, Grindstaff TL. Lumbar instability: an evolving and challenging concept. J Man Manip Ther. 2010 Mar;18(l):9-14. doi: 10.1179/106698110X1 2595770849443. PMID: 21655418; PMCID: PMC3103111.
14. Schinhan M, Bijak M, Unger E, Nau T. Electromyographic study of the popliteus muscle in the dynamic stabilization of the posterolateral comer structures of the knee. Am J Sports Med. 2011 Jan;39(l): 173-9. doi: 10.1177/0363546510377448. Epub 2010 Aug 31. PMID: 20807859.
15. Van Linge B, Mulder JD. Function of the supraspinatus muscle and its relation to the supraspinatus syndrome: an experimental study in man. J Bone Joint Surg Br. 1963 Nov;45(4):750-4. PMID: 14074328.
16. Roth, GB. Matrix Repatterning Practitioner Manual. Matrix Institute: Toronto; 2022.