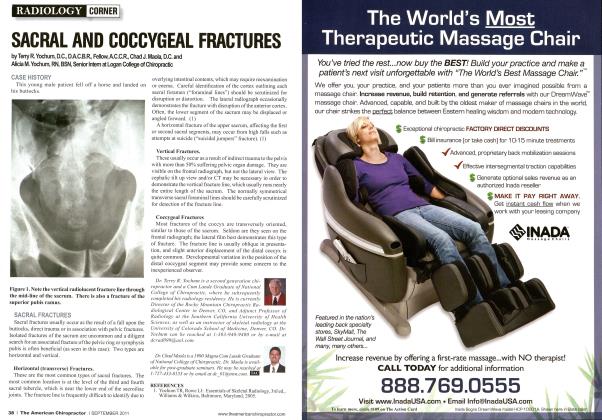
History: This 60-year-old male patient presents with acute lower thoracic pain alter a fall while skiing. Axial flexion compression force occurred during this fall. The radiographic examination demonstrates how many compression fractures? Are these compression fractures benign or malignant? DISCUSSION Compression fractures of the lumbar spine are the result of a combination of truncal flexion and axial compression. The extent of the vertebral compression and degree of comminution arc dependent upon the severity of the force applied and the relative strength of the vertebra. In the aging and geriatric patient with osteoporosis, compression fractures are quite common. The most common segmental levels to develop compression fractures are T12, LI and L2.u Radiojjrnphic signs of vertebral compression fracture include a step defect, wedge deformity, linear zone of condensation, displaced endplate, paraspinal edema, and abdominal ileus.1-2-1 The Step Defect. Since the anterior aspect of the vertebral body is under the greatest stress, the first bony injury to occur is a buckling of the anterior cortex, usually near the superior vertebral end-plate. This sign is best seen on the lateral view as a sharp step off of the anterosu-perior vertebral margin along the smooth concave edge of the vertebral body. In subtle compression fractures, the "step" defect may be the only radiographic sign of fracture. Anatomically, the actual step off defonnity represents the anteriorly displaced corner of the superior vertebral cortex. As the superior endplate is compressed in flexion, a sliding forward of the vertebral endplate occurs, creating this roentgen sign.1 Wedge Defonnity. In most compression fractures, an anterior depression of the vertebral body occurs, creating a triangular wedge shape. The posterior vertebral height remains uncompromised, differentiating a traumatic fracture from a pathological fracture. This wedging may create angular kyphosis in the adjacent area. It has been estimated that a 20 percent or greater loss in anterior height is required before the defonnity is readily apparent on conventional lateral radiographs of the spine.1 Linear While Band of Condensation (Zone oflmpaction). Occasionally, a band of radiopacity may be seen just below the vertebral endplate that has been fractured. The ladiopaque band represents the early site of bone impaction following a forceful flexion injury where the bones are driven together. Callus formation adds to the density of the radiopaque band later, in the healing stage of the fracture injury. This radiographic sign is striking when present; however, it is an unreliable sign, since it is not present as often as might be expected. Its presence, however, denotes a fracture of recent origin (less than 2 months' duration).1-1 Disruption in the Vertebral Endplate. A sharp disruption in the fractured vertebral endplate may be seen with spinal compression fracture. This may be difficult to perceive on plain films and tomography provides the definitive means to identification. The edges of the disruption arc often jagged and irregular.u Paraspinal Edema. In cases of extensive trauma, unilateral or bilateral paraspinal masses may occur which represent hemorrhage. These are best seen in the thoracic spine on the anteroposterior projection, but may occur adjacent to the lumbar spine, creating asymmetrical densities or bulges in the psoas margins.1-' Determining an Old versus a New Compression Fracture Since the wedge shape deformity of the vertebral body persists after the compression fracture heals, additional roentgen signs are necessary to evaluate the time status of a compression fracture. The presence of a "step" defect and the white band of condensation are signs of an active or current fracture (less than 2 months old). These two roentgen signs will vanish once the fracture totally heals, which may be as long as 3 months in the adult spine. When the question of presence or recent origin of the fracture arises, a radionuclide bone scan may be helpful. Such scans are positive (hot) with recent fractures undergoing active repair. These scans may stay positive (hot or warm) for as long as 18 months to 2 years following injury. This complicates the evaluation of a patient who has been injured previously (within 2 years). A bone scan may not prove helpful in this type of presentation.UJ Additionally, MRI scans are the most accurate way of determining whether a fracture is old or new. Bone marrow edema will be present in recent fractures of 6 weeks or less duration and is more accurate than a bone scan to determine the chronology of a compression fracture anywhere in the spine. See References on Pg 64 Dr. Terry R. Yochum is a second generation chiropractor and a Cum Laude Graduate of the National College of Chiropractic, where he subsequently completed his radiology residency. lie is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology at the University of Colorado School of Medicine, Denver, CO. Dr. Yochuin can he reached at 303-940-9400 or by e-mail at dcrai/099(waol.com. Dr. Chad J. Maola is a 1990 Mag-na Cum Laude Graduate of the National College of Chiropractic. Dr. Maola is a Chiropractic Orthopedist and is available for post-graduate seminars. He may be reached at 303-690-8503 or e-mail DCJJKcymsn. com. RADIOLOGY CORNER Compression Fractures-Pg. 16 by Terry R. Yochum, D.C., D.A.C.B.R., Fellow, A.C.C.R., and Chad J. Maola, D.C. Yochum TR, Rowe LJ, Essentials of Skeletal Radiology, 3rd ed. Lippincott, Williams and Wilkins, Baltimore, 2005. Roof R, A Study of Mechanics of Spinal Inju ries, J Bone Joint Surg. (Br) 42:810,1960. Gehweiler JA, et al, The Radiology of Verte bral Trauma, Philadelphia, W.B. Saunders, 1980.