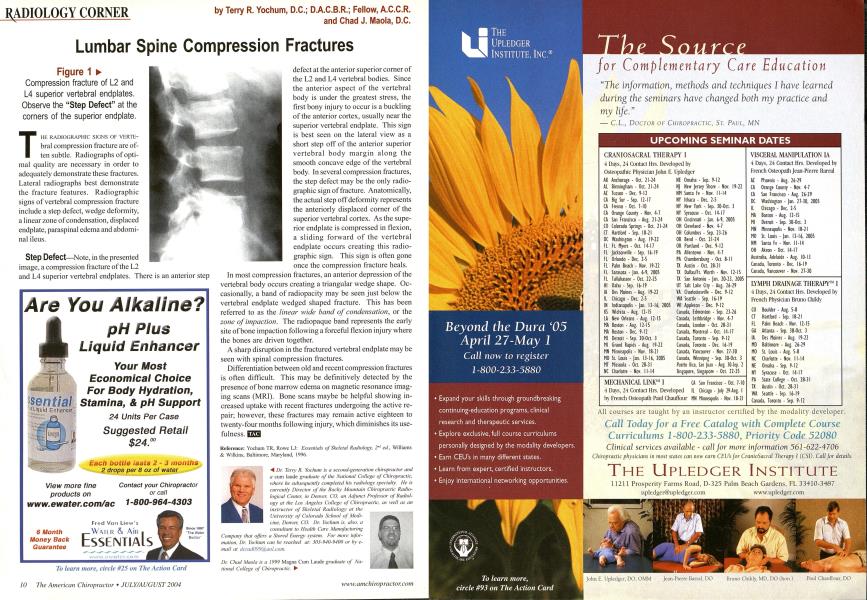
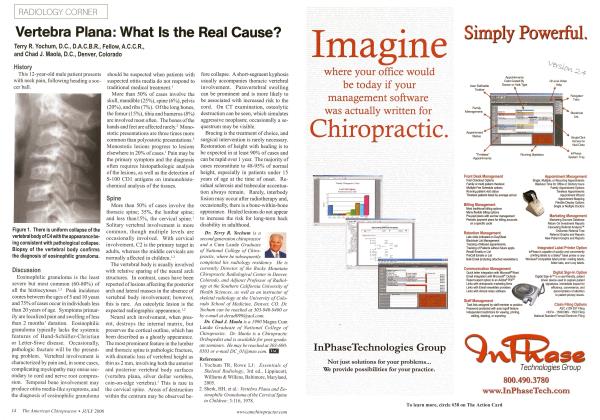
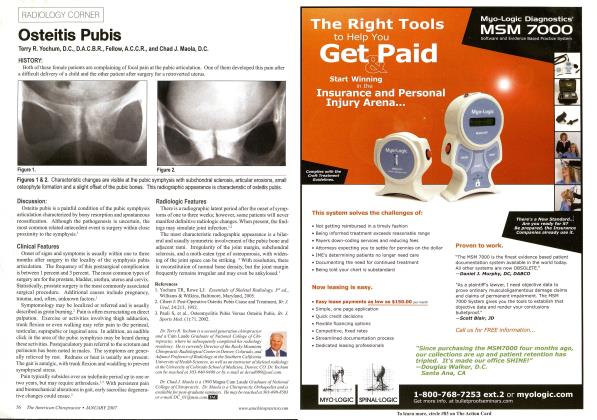
Figure 1 ► Compression fracture of L2 and L4 superior vertebral endplates. Observe the "Step Defect" at the corners of the superior endplate. Till: RADIOCJRAPHIC SIGNS OF VERTE-bral compression fracture are often subtle. Radiographs of optimal quality are necessary in order to adequately demonstrate these fractures. Lateral radiographs best demonstrate the fracture features. Radiographic signs of vertebral compression fracture include a step defect, wedge deformity, a linear zone of condensation, displaced endplate, paraspinal edema and abdominal ileus. Step Defect—Note, in the presented image, a compression fracture of the L2 and L4 superior vertebral endplates. There is an anterior step defect at the anterior superior corner of the L2 and L4 vertebral bodies. Since the anterior aspect of the vertebral body is under the greatest stress, the first bony injury to occur is a buckling of the anterior cortex, usually near the superior vertebral endplate. This sign is best seen on the lateral view as a short step off of the anterior superior vertebral body margin along the smooth concave edge of the vertebral body. In several compression fractures, the step defect may be the only radio-graphic sign of fracture. Anatomically, the actual step off deformity represents the anteriorly displaced corner of the superior vertebral cortex. As the superior endplate is compressed in flexion, a sliding forward of the vertebral endplate occurs creating this radio-graphic sign. This sign is often gone once the compression fracture heals. In most compression fractures, an anterior depression of the vertebral body occurs creating a triangular wedge shape. Occasionally, a band of radiopacity may be seen just below the vertebral endplate wedged shaped fracture. This has been referred to as the linear wide band of condensation, or the zone of impaction. The radiopaque band represents the early site of bone impaction following a forceful flexion injury where the bones are driven together. A sharp disruption in the fractured vertebral endplate may be seen with spinal compression fractures. Differentiation between old and recent compression fractures is often difficult. This may be definitively detected by the presence of bone marrow edema on magnetic resonance imaging scans (MRI). Bone scans maybe be helpful showing increased uptake with recent fractures undergoing the active repair; however, these fractures may remain active eighteen to twenty-four months following injury, which diminishes its use- Kcfcrcncc: Yochuni TR. Rowc LJ: Essentials of Skeletal Radiology, 2nd ed., Williams & Wilkins, Baltimore, Maryland, 1996. A Dr. Terry R. Yochum is a second-generation chiropractor and a cum laude graduate of the National College of Chiropractic, where he subsequently completed his radiology specialty. He is currently Director of the Rockv Mountain Chiropractic Radiological Center, in Denver, CO. an Adjunct Professor of Radiology at the Los Angeles College of Chiropractic, as well as an instructor of Skeletal Radiology at the University of Colorado School of Medicine, Denver. CO. Dr. Yochum is. also, a consultant to Health Care Manufacturing Company thai offers a Stored Energy system. For more information. Dr. Yuclmm can he reached at: 303-940-9400 or by e-mail al JcrMtOV9%a0l.com. Dr. Chad Maola is a 1999 Magna Cum Laude graduate of National College of Chiropractic. ►