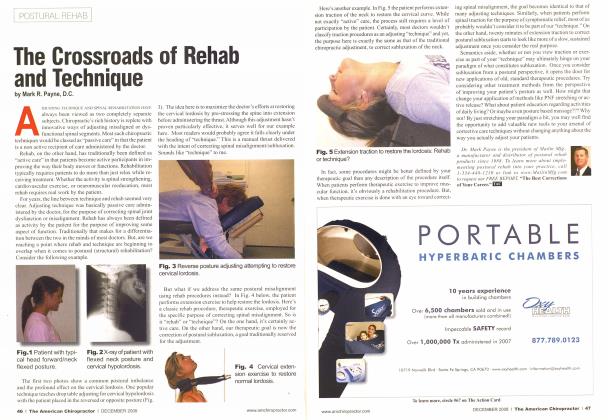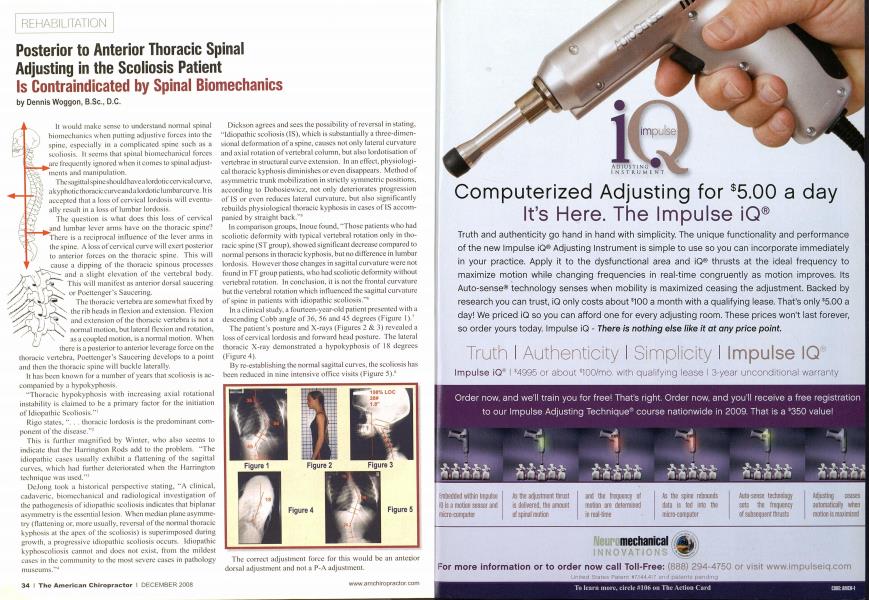
It would make sense to understand normal spinal biomechanics when putting adjustive forces into the spine, especially in a complicated spine such as a scoliosis. It seems that spinal biomechanical forces are frequently ignored when it conies to spinal adjustments and manipulation. The sagittal spine should havea lordotic cervical curve, a kyphotic thoracic curveandalordotielumbareurve. It is accepted that a loss of cervical lordosis will eventually result in a loss of lumbar lordosis. The question is what does this loss of cervical and lumbar lever arms have on the thoracic spine? There is a reciprocal influence of the lever arms in the spine. A loss of cervical curse will exert posterior to anterior forces on the thoracic spine. This will cause a dipping of the thoracic spinous processes and a slight elevation of the vertebral body. This will manifest as anterior dorsal saucering or Poettenger"s Saucering. The thoracic vertebra are somewhat fixed by - the rib heads in flexion and extension. Flexion "■ and extension of the thoracic vertebra is not a . normal motion, but lateral flexion and rotation. as a coupled motion, is a normal motion. When there is a posterior to anterior leverage force on the thoracic vertebra. Poettenger's Saucering develops to a point and then the thoracic spine will buckle laterally. It has been known for a number of years that scoliosis is accompanied by a hypokyphosis. "Thoracic hypokyphosis with increasing axial rotational instability is claimed to be a primary factor for the initiation of Idiopathic Scoliosis."1 Rigo states. ". . . thoracic lordosis is the predominant component of the disease."2 This is further magnified by Winter, who also seems to indicate that the Harrington Rods add to the problem. "The idiopathic cases usually exhibit a flattening of the sagittal curves, which had further deteriorated when the Harrington technique was used.'"' DeJong took a historical perspective stating, "A clinical, cadaveric, biomechanieal and radiological investigation of the pathogenesis ofidiopathic scoliosis indicates that biplanar asymmetry is the essential lesion. When median plane asymmetry (flattening or. more usually, reversal of the normal thoracic kyphosis at the apex of the scoliosis) is superimposed during growth, a progressive idiopathic scoliosis occurs. Idiopathic kyphoscoliosis cannot and does not exist, from the mildest cases in the community to the most severe cases in pathology museums."4 Dickson agrees and sees the possibility of reversal in stating, "Idiopathic scoliosis (IS), which is substantially a three-dimensional deformation of a spine, causes not only lateral curvature and axial rotation of vertebral column, but also lordotisation of vertebrae in structural curve extension. In an effect, physiological thoracic kyphosis diminishes or even disappears. Method of asymmetric trunk mobilization in strictly symmetric positions, according to Dobosiewicz, not only deteriorates progression of IS or even reduces lateral curvature, but also significantly rebuilds physiological thoracic kyphosis in cases of IS accompanied by straight back."5 In comparison groups. Inoue found. "Those patients who had scoliotic deformity with typical vertebral rotation only in thoracic spine (STgroup), showed significant decrease compared to normal persons in thoracic kyphosis. but no difference in lumbar lordosis. However those changes in sagittal curvature were not found in FT group patients, who had scoliotic deformity without vertebral rotation. In conclusion, it is not the frontal curvature but the vertebral rotation which influenced the sagittal curvature of spine in patients with idiopathic scoliosis."6 In a clinical study, a fourteen-year-old patient presented with a descending Cobb angle of 36, 56 and 45 degrees (Figure 1)." The patient's posture and X-rays (Figures 2 & 3) revealed a loss of cervical lordosis and forward head posture. The lateral thoracic X-ray demonstrated a hypokyphosis of 18 degrees (Figure 4). By re-establishing the normal sagittal curves, the scoliosis has been reduced in nine intensive office visits (Figure 5).s The correct adjustment force for this vvoulci be an anterior dorsal adjustment and not a P-A adjustment. It would appear that a loss ofthe cervical lordosis can cause an anterior dorsal saucering resulting in a lateral bending motion of the thoracic spine. Based on this, posterior to anterior thoracic adjusting in these areas would appear to be contraindicated. This would also apply to the scoliosis patient or the potential scoliosis patient in regard to P-A thoracic adjusting as well as adjusting on the "high side of the rainbow." As Hippocrates said. ■"First, do no harm." For further information, contact Dr. Dennis H'oggwt ut www.dear-instilute.org. References 1. Sagittal configuration ofthe spine in girls with idiopathic scoliosis: progressing rather than initiating factor. Rigo M. Queia-Salva (i. Villagers M. Elena Salva Spinal Deformi ties Rehabilitation Institute. Via Augusta 185, 08021 Barcelona, Spain. Stud Health Technol Inform. 2006:123:90-4. Excessive thoracic lordosis and loss of pulmo nary function in patients with idiopathic sco liosis. Winter RB. Lovell WW, Moe.111. Bone Joint Surg Am. 1975 Oct:57(7):972-7. Sagittal plane correction in idiopathic scolio sis. de JongeT. Duboussct JF, IllesT. Univer sity of Pecs. Faculty of Medicine. Department ol( )rlhopedic Surgery, Pecs. Hungary. Spine. 2002 Apr l:27(7):761. For the complete list of references far llii: article, please visit our wehsile at www.theamericanchiropractor.coni