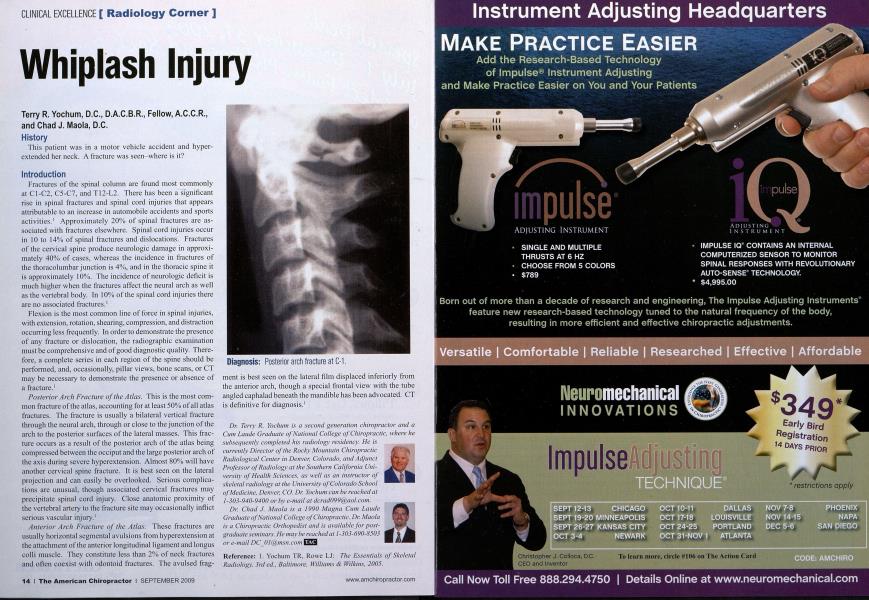
History This patient was in a motor vehicle accident and hyper-extended her neck. A fracture was seen-where is it? Introduction Fractures of the spinal column are found most commonly at C1-C2, C5-C7, and T12-L2. There has been a significant rise in spinal fractures and spinal cord injuries that appears attributable to an increase in automobile accidents and sports activities.' Approximately 20% of spinal fractures are associated with fractures elsewhere. Spinal cord injuries occur in 10 to 14% of spinal fractures and dislocations. Fractures of the cervical spine produce neurologic damage in approximately 40% of cases, whereas the incidence in fractures of the thoracolumbar junction is 4%, and in the thoracic spine it is approximately 10%. The incidence of neurologic deficit is much higher when the fractures affect the neural arch as well as the vertebral body. In 10% of the spinal cord injuries there are no associated fractures.1 Flexion is the most common line of force in spinal injuries, with extension, rotation, shearing, compression, and distraction occurring less frequently. In order to demonstrate the presence of any fracture or dislocation, the radiographic examination must be comprehensive and of good diagnostic quality. Therefore, a complete series in each region of the spine should be performed, and, occasionally, pillar views, bone scans, or CT may be necessary to demonstrate the presence or absence of a fracture.1 Posterior Arch Fracture of the Atlas. This is the most common fracture of the atlas, accounting for at least 50% of all atlas fractures. The fracture is usually a bilateral vertical fracture through the neural arch, through or close to the junction of the arch to the posterior surfaces of the lateral masses. This fracture occurs as a result of the posterior arch of the atlas being compressed between the occiput and the large posterior arch of the axis during severe hyperextension. Almost 80% will have another cervical spine fracture. It is best seen on the lateral projection and can easily be overlooked. Serious complications are unusual, though associated cervical fractures may precipitate spinal cord injury. Close anatomic proximity of the vertebral artery to the fracture site may occasionally inflict serious vascular injury.' Anterior Arch Fracture of the Atlas. These fractures are usually horizontal scgmcntal avulsions from hyperextension at the attachment of the anterior longitudinal ligament and longus colli muscle. They constitute less than 2% of neck fractures and often coexist with odontoid fractures. The avulsed frag- ment is best seen on the lateral film displaced inferiorly from the anterior arch, though a special frontal view with the tube angled caphalad beneath the mandible has been advocated. CT is definitive for diagnosis.1 Dr. Terry R. Yochum is a second generation chiropractor and a Cum Laudc Graduate of National College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology' at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology at the University of Colorado School of Medicine, Denver. CO. Dr. Yochum can be reached at 1-303-940-9400 or by e-mail at [email protected]. Dr. Chad J. Maola is a 1990 Magna Cum Laude Graduate of National College of Chiropractic. Dr. Maola is a Chiropractic Orthopedist and is available for postgraduate seminars. He may be reached at 1-303-690-8503 or e-mail [email protected] | Reference: 1. Yochum TR, Rowe LJ: The Essentials of Skeletal Radiology, 3rd ed., Baltimore, Williams & Wilkins, 2005.