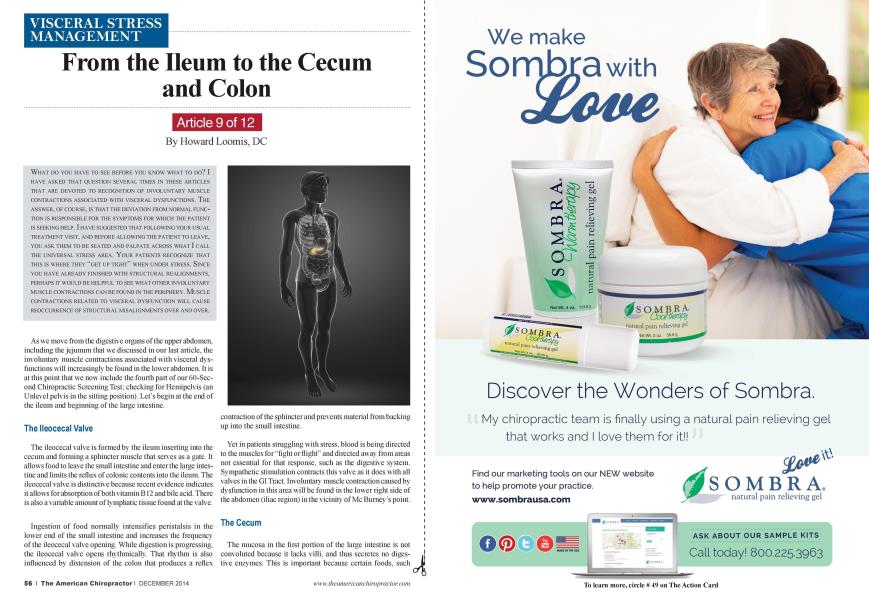
Article 9 of 12 What do you have to see before you know what to do? I HAVE ASKED THAT QUESTION SEVERAL TIMES IN THESE ARTICLES THAT ARE DEVOTED TO RECOGNITION OF INVOLUNTARY MUSCLE CONTRACTIONS ASSOCIATED WITH VISCERAL DYSFUNCTIONS. THE ANSWER. OF COURSE, IS THAT THE DEVIATION FROM NORMAL FUNCTION IS RESPONSIBLE FOR THE SYMPTOMS FOR WHICH THE PATIENT IS SEEKING HELP. I HAVE SUGGESTED THAT FOLLOWING YOUR USUAL TREATMENT VISIT, AND BEFORE ALLOWING THE PATIENT TO LEAVE, YOU ASK THEM TO BE SEATED AND PALPATE ACROSS WHAT I CALL THE UNIVERSAL STRESS AREA. YOUR PATIENTS RECOGNIZE THAT THIS IS WHERE THEY "GET UP TIGHT" WHEN UNDER STRESS. SlNCE YOU HAVE ALREADY FINISHED WITH STRUCTURAL REALIGNMENTS, PERHAPS IT WOULD BE HELPFUL TO SEE WHAT OTHER INVOLUNTARY MUSCLE CONTRACTIONS CAN BE FOUND IN THE PERIPHERY. MUSCLE CONTRACTIONS RELATED TO VISCERAL DYSFUNCTION WILL CAUSE REOCCURRENCE OF STRUCTURAL MISALIGNMENTS OVER AND OVER. As we move from the digestive organs of the upper abdomen, including the jejunum that we discussed in our last article, the involuntary muscle contractions associated with visceral dysfunctions will increasingly be found in the lower abdomen. It is at this point that we now include the fourth part of our 60-Scc-ond Chiropractic Screening Test: checking for Hemipelvis (an Unlcvcl pelvis in the sitting position). Lct"s begin at the end of the ileum and beginning of the large intestine. The lleocecal Valve The ileocecal valve is formed by the ileum inserting into the cecum and forming a sphincter muscle that serves as a gate. It allows food to leave the small intestine and enter the large intestine and limits the reflux of colonic contents into the ileum. The ileocecal valve is distinctive because recent evidence indicates it allows for absorption of both vitamin B12 and bile acid. There is also a variable amount of lymphatic tissue found at the valve. Ingcstion of food normally intensifies peristalsis in the lower end of the small intestine and increases the frequency of the ileocecal valve opening. While digestion is progressing, the ileocecal valve opens rhythmically. That rhythm is also influenced by distension of the colon that produces a reflex contraction of the sphincter and prevents material from backing up into the small intestine. Yet in patients struggling with stress, blood is being directed to the muscles for "fight or flight" and directed away from areas not essential for that response, such as the digestive system. Sympathetic stimulation contracts this valve as it does with all valves in the GI Tract. Involuntary muscle contraction caused by dysfunction in this area will be found in the lower right side of the abdomen (iliac region) in the vicinity of Me Burncy"s point. The Cecum The mucosa in the first portion of the large intestine is not convoluted because it lacks villi. and thus secretes no digestive enzymes. This is important because certain foods, such a as beans, contain types of carbohydrates that arc not digested by intestinal enzymes. There are large quantities of parasitic microorganisms living in the cccuni (not indigenous to the human body) that thrive on these compounds. Their various end products contribute to production of intestinal gas. The Appendix The cccuni contains the appendix attached to its inferior surface and has no apparent digestive function, but contains a small amount of mucosa-associatcd lymphoid tissue. This gives the appendix an undetermined role in immunity. It is interesting to note, it has been theorized by researchers that prehistorically the appendix functioned immunologically to protect against parasitic infestation. I recall that, in the 1970s. an ostcopathic hospital in Michigan studied 100 surgically removed appendages. All 100 contained parasites. By the way. the classic symptoms of appendicitis usually begin as involuntary muscle contractions and dull pain near the navel or the upper abdomen that becomes sharp when it moves to the lower right abdomen. The abdominal discomfort is at first not confined to one spot and is difficult to pinpoint, similarly to colic. But when the pain becomes sharp, moves to the right, and fever begins, it is time for medical intervention. The appendix is known to be important in fetal life as it contains endocrine cells that release biogenic amines and peptide hormones important for homeostasis during early growth and development. The Colon Follow ing the cccum is the colon, which consists of three relatively straight segments. It is here that abdominal palpation for involuntary muscle contraction becomes very revealing. Dysfunction in the ascending, transverse, and descending portions in particular affect different areas of the lower abdominal muscles. The last section, the sigmoid colon, is S-shapcd and empties into the rectum. Equally important, different areas of the spine are affected due to differences in parasympathctic innervation. We will examine those relationships next month. For now we will concentrate on the functions of the colon. The large intestine is roughly 2.5 inches in diameter and forms the last 4 feet of the gastrointestinal tract. Although the large intestine has a greater diameter than the small intestine, it is only about half as long. Its epithelial surface secretions consist mostly of mucus and its primary function is to store and concentrate fecal material prior to defecation. The primary role of the colon in absorption is its active transport of sodium and water back to the blood from the gut. If fecal material remains in the large intestine for long periods of time, almost all of the water is absorbed and dry fecal pellets are left behind. This occurs when passage of the fecal material is delayed by the action of microorganisms. Mixing Contractions in the Colon Contractions in the large intestine resemble those of the small intestine, with one exception: the outward bulging of the relaxed segments between the constricted rings. These bulges or sacs arc called haustra. and result from the simultaneous contraction of longitudinal and circular muscle. This type of contraction serves primarily to mix colon contents, but it also propels fecal material up the ascending colon and into the transverse colon. Three to four times a day. generally following a meal, a wave of intense contraction known as a mass movement spreads rapidly over the colon and toward the rectum. This usually coincides with the gastroileal reflex that occurs when food is ingested. These contractions of the circular smooth muscle produce a propelling motion considerably slower than that of the small intestine. A contraction may occur only once every 30 minutes. Because of this slow movement, material entering the colon from the small intestine can remain as long as 18 to 24 hours. This provides enough time for bacteria to grow and multiply. Peristaltic contractions occur less frequently. These contractions arc mass movements and generally occur no more than two or three times a day. occurring most commonly during or shortly after a meal. The mass movement wave is characteristically prolonged. It lasts two to four minutes and rapidly transfers the contents of the proximal colon to the distal colon. These movements are often followed by a desire to defecate. Recall that peristaltic contractions arc diminished in stress. We will continue our discussion of the large intestine next month and discuss the effect of an unlcvcl pelvis in the sitting position and its effect on bowel elimination. Dr. Howard Loomis has an extensive background in enzymes and enzyme supplements. He is the founder and president of Enzyme Formulations®, Inc. His knowledge of physiology, biochemistry, and enzymology has made him a sought-after speaker and a prolific writer. Dr. Loomis published EXZYMES: The Key to Health in 1999. Contact info: 6421 Enterprise Lane, Madison, WI 53719, cuslomerservicefdloomisinslitule.com