Kienböck’s DISEASE
RADIOLOGY
Terry R. Yochum,
Case History:
This adult patient presents with persistent right wrist pain after multiple episodes of trauma the wrist.
General Considerations
In 1910, Dr. Robert Kienböck first described
avascular necrosis ofthe carpal lunate in detail. Alternate terms include Kienböck’s disease, lunate osteochondrosis, and lunate malacia.
Clinical Features
A definite predilection is apparent in males over females of up to 9:1. The disorder is most commonly observed in the 20 to 40 age group. A history of previous acute trauma or occupational excessive hand use, especially ofthe dominant extremity, may be obtained, but a great many individuals have no known association. MRI would demonstrate findings much earlier than conventional radio graphs. With progression, however, a number of signs become evident on plain fi1m/12)
Pathological Features
The histopathological picture is that of avascular necrosis. Resorption, deposition, fragmentation, and collapse typify the osseous necrosis. The isolation of contributing etiologies has been inconclusive, although trauma appears to be a prominent factor. Vascular studies ofthe lunate suggest possible vulnerability. A short ulna (negative ulnar variance) is found in up to 75% of cases, which may augment mechanical stresses between the lunate and radius and predispose to vascular impediment/1,2)
Radiological Features
The radiographic examination may be initially unrewarding for many months. If the patient has not used the affected hand because of symptoms, disuse osteoporosis of all adjacent bones will accentuate the density ofthe lunate, which remains normal due to its lack of blood supply. With progression, however, a number of signs become evident/1’2)
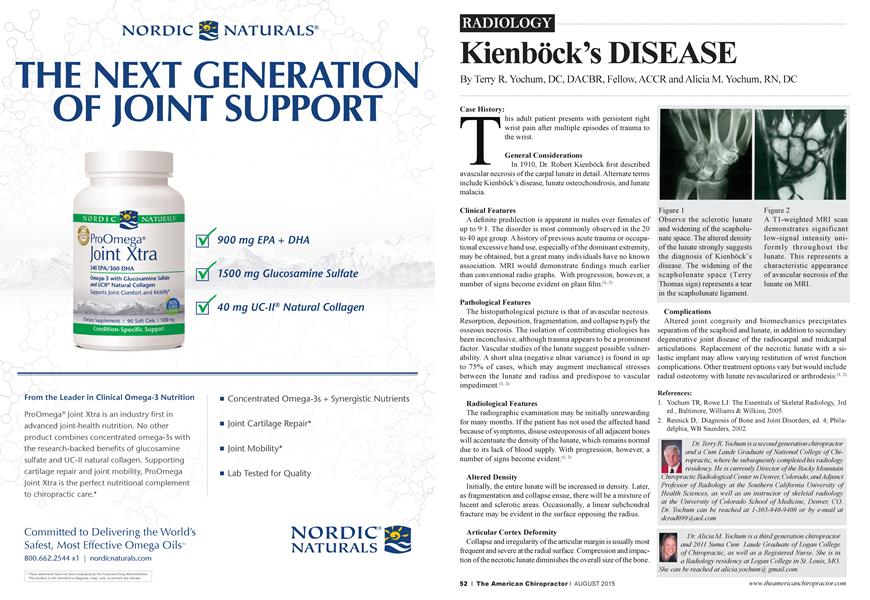
Altered Density
Initially, the entire lunate will be increased in density. Later, as fragmentation and collapse ensue, there will be a mixture of lucent and sclerotic areas. Occasionally, a linear subchondral fracture may be evident in the surface opposing the radius.
Articular Cortex Deformity
Collapse and irregularity ofthe articular margin is usually most frequent and severe at the radial surface. Compression and impaction ofthe necrotic lunate diminishes the overall size ofthe bone.
Complications
Altered joint congruity and biomechanics precipitates separation ofthe scaphoid and lunate, in addition to secondary degenerative joint disease of the radiocarpal and midcarpal articulations. Replacement of the necrotic lunate with a silastic implant may allow varying restitution of wrist function complications. Other treatment options vary but would include radial osteotomy with lunate revascularized or arthrodesis/1-2)
References:
1. Yochum TR, Rowe LJ: The Essentials of Skeletal Radiology, 3rd ed., Baltimore, Williams & Wilkins, 2005.
2. Resnick D,: Diagnosis of Bone and Joint Disorders, ed. 4, Philadelphia, WB Saunders, 2002.
Dr. Terry R. Yochum is a second generation chiropractor and a Cum Laude Graduate of National College of Chiropractic, where he subsequently completed his radiology residency. He is currently Director of the Rocky Mountain Chiropractic Radiological Center in Denver, Colorado, and Adjunct Professor of Radiology at the Southern California University of Health Sciences, as well as an instructor of skeletal radiology at the University of Colorado School of Medicine, Denver, CO. Dr Yochum can be reached at 1-303-940-9400 or by e-mail at dcrad099(aaol. com
Dr Alicia M. Yochum is a third generation chiropractor and 2011 Suma Cum Laude Graduate of Logan College of Chiropractic, as well as a Registered Nurse. She is in a Radiology residency at Logan College in St. Louis, MO. She can be reached at alicia.yochunkxf gmail.com.