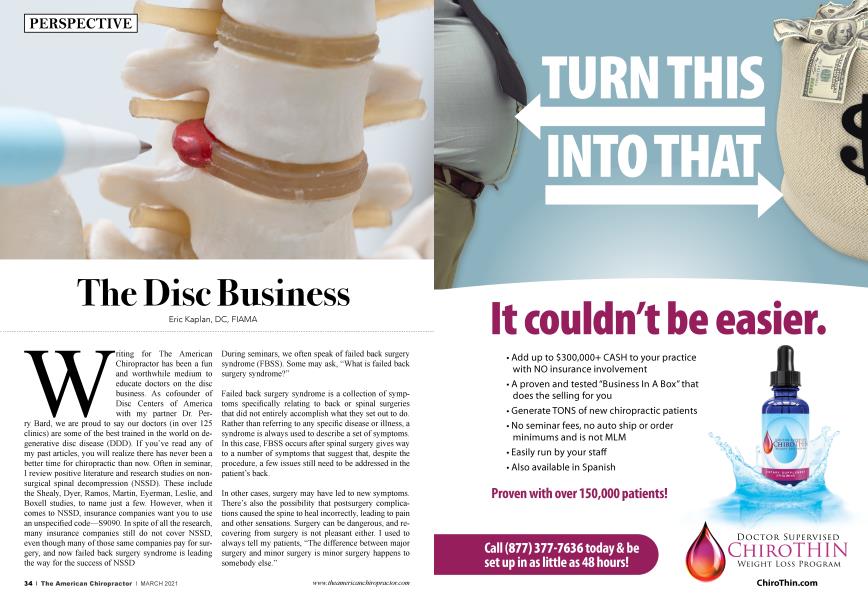
Writing for The American Chiropractor has been a fun and worthwhile medium to educate doctors on the disc business. As co-founder of Disc Centers of America with my partner Dr. Perry Bard, we are proud to say our doctors (in over 125 clinics) are some of the best trained in the world on degenerative disc disease (DDD). If you’ve read any of my past articles, you will realize there has never been a better time for chiropractic than now. Often in seminars, I review positive literature and research studies on nonsurgical spinal decompression (NSSD). These include the Shealy, Dyer, Ramos, Martin, Eyerman, Leslie, and Boxell studies, to name just a few. However, when it comes to NSSD, insurance companies want you to use an unspecified code—S9090. In spite of all the research, many insurance companies still do not cover NSSD, even though many of those same companies pay for surgery, and now failed back surgery syndrome is leading the way for the success of NSSD During seminars, we often speak of failed back surgery syndrome (FBSS). Some may ask, “What is failed back surgery syndrome?”
Failed back surgery syndrome is a collection of symptoms specifically relating to back or spinal surgeries that did not entirely accomplish what they set out to do. Rather than referring to any specific disease or illness, a syndrome is always used to describe a set of symptoms. In this case, FBSS occurs after spinal surgery gives way to a number of symptoms that suggest that, despite the procedure, a few issues still need to be addressed in the patient’s back.
In other cases, surgery may have led to new symptoms. There’s also the possibility that postsurgery complications caused the spine to heal incorrectly, leading to pain and other sensations. Surgery can be dangerous, and recovering from surgery is not pleasant either. I used to always tell my patients, “The difference between major surgery and minor surgery is minor surgery happens to somebody else.”
Spinal surgeries are quite complicated, and even when taking all possible measures, many studies show a 40% or greater failure rate. Such a failure rate indicates that postsurgery pain is equal to or greater than before surgery.
Often the problem develops months after surgery. All patients will heal with scar tissue after back surgeries because that is the only way to heal. Although scar tissue is often clinically the reason given for continued pain after surgery, it is probably rarely the cause of initial postoperative pain. It is unlikely that the addition of scar tissue has any clinical relevance immediately following surgery. This happens over time, particularly for patients who have similar pain postoperatively to what they had before surgery. That comes later. They can cut and remove parts of the anatomy, but you can’t surgically remove pain.
If it were me, this would scare the heck out of me, but Americans undergo back surgery daily, more than any other country. As chiropractors, our responsibility is to educate and eliminate the need for unnecessary surgeries. Approximately one in five patients who undergo spinal surgery for a degenerative disorder returns for a revision procedure—yes, a second operation. Even when the fusion is sometimes deemed to be “radiologically perfect” (i.e., on an X-ray the vertebrae have grown together and the hardware is positioned correctly), the fusion itself imposes increased stress at other vertebral segments. That often results in “adjacent segment deterioration,” a condition where the vertebral level above or below degrades, causing more pain, or scar tissue causes affects other nerves, resulting in severe pain.
Some studies show that a second back surgery may have only a 30% chance of success, which are not good odds. It is again estimated that the prognosis drops to 15% for a third back surgery, and 5% for a fourth. Tiger Woods just had his fifth back surgery.
Oregon Health and Science University spine medicine researcher Roger Chou believes that surgeons should be required to reveal the odds to their patients before going forward with a procedure. “If [the surgeon] said, ‘Yes, we can do this $70,000 surgery, but you know, there’s still more than a 50% chance that you’re going to have a lot of pain, and you still won’t be able to work, and you’re going to need pain medicine, and you’ll have complications related to the surgery'—and all this is well documented— then most people would say, ‘I don’t want it.’”
During my 40 years as a chiropractor, I cannot count the number of stories told by doctors of patients who admitted that they chose injections, surgery, and pharmaceutical pain management NSSD or Chiropractic, simply because those medical interventions were covered by insurance (and seemed quick and easy). On the contrary, cognitive-behavioral psychology sessions and intensive exercise were difficult to find, had to be paid for out of pocket, and took lots of time. They never considered the pain factor, never considered the progression of the disease, and never considered the time for lost work or the cost of rehabilitation and medication.
Modern medicine has continually looked for a less invasive approach to back surgery, but we know that surgery is surgery. Minimally invasive spinal surgery didn’t become a big deal until marketers started selling it in the early 1980s. That’s when physicians tested a method of injecting chymopapain, an enzyme derived from the latex of the papaya tree, into the disc’s gelatinous interior.
I remember patients thinking chymopapain was the cure for back pain until I explained the procedure and the facts. The papaya enzyme was supposed to dissolve proteins inside the disc, which softened and shrank in size, thereby reducing pressure on the spinal nerve root.
When the FDA approved chymopapain in 1983 for use in chemonucleolysis, the American Academy of Orthopaedic Surgeons endorsed it. Because this procedure was expected to eliminate half of conventional microdiscectomies, (and thereby cut deeply into revenue), 7,000 doctors showed up for one-day training sessions and treated tens of thousands of patients over the next few years. For a relatively small number of patients, chymopapain was sometimes accidentally injected into the patient’s spinal canal instead of finding its way into the disc, injuring soft tissues and nerves, and causing pain and paralysis.
Even when chemonucleolysis was performed correctly, some patients experienced allergic reactions, including anaphylactic shock, which could be fatal. Almost 10 years after chymopapain was introduced, a study showed that chemonucleolysis was not what it had been cracked up to be, perhaps because it had been poorly administered. In reality, it was hardly more effective than a placebo injection of inactive saline, and at that point, the procedure was shelved.
It’s funny how the world looks for a minimally invasive approach to spinal surgery and ignores NSSD, the true alternative, safe approach in lieu of any surgery. Whether it is chymopapain or laser spinal surgery, most of these approaches continually fail, but study after study shows the effectiveness of NSSD. The laser spinal surgery craze took hold in the mid-1990s, but it took more than a decade for a well-designed Cochrane Collaboration review to show that the minimally invasive procedure resulted in higher levels of nerve root injury, dural tears, and reoperation rates, and therefore was not safer than a conventional microdiscectomy. The minimally invasive group had a 38% revision rate, more than double that of the group that underwent the standard procedure. Patients who had conventional microdiscectomy recovered faster than those in the laser surgery group, and they required fewer than half as many return trips to the operating suite.
The Laser Spine Institute, which once ran a nationwide chain of surgery centers that specialized in “minimally invasive” spinal procedures, has abruptly ceased operations due to financial problems. The company had four remaining surgery centers in St. Louis, Missouri; Cincinnati, Ohio; Scottsdale, Arizona; and Tampa, Florida, where it is headquartered. It recently closed three other surgery centers in an effort to control costs and restructure.
Despite “significant cost saving” in recent months, the Laser Spine Institute said in a news release that it was “unable to attract the necessary financing” to continue operating while it sought Chapter 11 bankruptcy protection. About 600 employees were affected.
The Laser Spine Institute treated patients with neck and back pain caused by spinal stenosis, degenerative disc disease, pinched nerves, bone spurs, herniated discs, sciatica, and other chronic conditions. Although it claimed to have a 98% patient satisfaction rate, the company was hit with dozens of malpractice lawsuits, including one by superstar wrestler Hulk Hogan, who claimed its treatments were ineffective and cost him $50 million in lost revenue. Hogan reportedly settled out of court for $10 million. Last year the family of a Pennsylvania woman who died hours after being discharged from a Laser Spine Institute surgery center was awarded $20 million in a wrongful death lawsuit.
A competing surgery center also sued the Laser Spine Institute for offering illegal incentives to patients, such as paying for their airfare and hotel expenses, which is prohibited under Medicare guidelines. Nine surgeons told Bloomberg Businessweek that the company was doing spinal surgeries that were often unnecessary or inappropriate.
Today we have ample evidence that spinal fusion can send a patient into a costly tailspin, and that neither spinal injections nor long-term opioid therapy is 100% effective and often contraindicated. As a result, new coverage approaches are emerging from the insurance industry. We are starting to see some companies pay for NSSD, even the VA. In addition, many are recommending classes in back-healthy disciplines such as tai chi and Feldenkrais.
It is up to us as chiropractors for how this might change in the future. Our job is to educate the insurance companies and educate the masses. There is an alternative to back surgery, and non-surgical spinal decompression seems to be the answer.
About the Author
Dr. Eric S. Kaplan, is President of DISC Centers of America, the largest group of Chiropractic clinics in the U.S.A., utilizing Non-Surgical Spinal Decompression. He has worked with two Presidents of the United States and two U.S. Surgeon Generals. He is CEO of Concierge Coaches, www.conciergecoaches.com, the #1 Chiropractic firm in Spinal Decompression and Neuropathy training nationwide. To read some of the research studies, go to DiscCentersofamerica.com. Or email him at [email protected]