The first year of chiropractic college is filled with an academic load that does not include much in the way of hands-on chiropractic. While that’s probably in everyone’s best interest, I remember being hungry to learn. Our zeal to get started being chiropractors was met with the very safe assignment of becoming observers of people. We were told to go to the mall and sit on the bench by the artificial plants in front of RadioShack and BuildA-Bear. We were instructed to discretely watch the way people walked and look for signs of postural stress. “See if you can find someone whose belt isn’t level. They have a high hip.”
Once proficient at detecting pelvic unleveling, we were charged with identifying the ever-so-common low shoulder. It soon became apparent that those were prevalent and easy to spot with a little practice. We graduated from hips and shoulders to limps and lurches, soon being able to tell where the pain was emanating from. That was the starting point of patient evaluation, and it opened our eyes to numerous indicators of postural and functional deficiencies.
One of the most fascinating features of these postural deviations is that shoulders and hips weren’t really the problem. Instead, issues were the result of postural imbalances often related to the feet. These distortion patterns have been summarized as the “five red flags” of excessive pronation, which can contribute significantly to biomechanical stress and lead to many painful conditions. Some of these are easy to see from a distance when you watch how people walk, and a couple of them will require a closer look.
The Importance of Gait and Foot Assessment in Chiropractic Care
My personal experience of having someone look at my gait and posture was after chiropractic college at a chiropractic convention. I had suffered numerous sports-related injuries and had developed low back pain that was becoming more persistent. Chiropractic care offered temporary relief, but something else was going on that wasn’t being addressed. My feet were identified as part of my injury experience, even though my feet never hurt. The clues were there all along, but evaluation of the feet and gait isn’t always part of a new patient exam.
What Is Normal Gait?
Let’s start with what is understood as normal walking gait. The walking gait cycle starts when the foot makes contact with the ground on the posterior lateral part of the calcaneus. The line of weight-bearing (center of pressure) moves from the lateral heel along the fifth metatarsal until the foot is in a full weight-bearing position, at which point the foot pronates, and the center of pressure travels medially across the metatarsal heads. Pronation of the foot is a tri-planar movement of the calcaneus and foot consisting of calcaneal eversion (frontal plane), abduction (transverse plane), and dorsiflexion (sagittal plane). At that point, the foot goes into the “toe-off phase.” The pressure then travels distally to the end of the first ray (big toe), where we toe-off and enter the swing phase of the gait cycle. During the swing phase, the foot supinates, which is an opposing movement of calcaneal inversion, adduction, and plantar flexion in the same planes.
With normal gait in mind, we can begin to observe visual clues that the gait cycle includes some functional variations that can be significant contributors to the clinical picture the patient presents.
Asymmetrical Heel Wear
The posterior lateral part of the heel makes contact with the ground, and when you look at your patient’s shoes, that’s where you will see a wear pattern. The posterior lateral heel is considered the normal location of wear based on the fact the calcaneus is inverted and adducted in the swing phase before making contact with the ground. Asymmetrical wear between the left and right shoe is the key finding here. If we see a difference in the wear pattern between the right and left foot, we will often see excessive foot flare on one side.
Foot Flare
When the foot makes contact with the ground, a small amount of external rotation of the foot occurs, also known as foot flare. According to the Fick angle, 12 to 18 degrees of foot flare is considered normal during the gait cycle. An angulation greater than that can be attributed to excessive pronation, which then also creates excessive external rotation of the knee and hip. This is the easiest of the five red flags to see during the gait cycle, but it is often also evident when the patient is standing.
Increased Q Angle
The Q angle is a line representing the resultant line of force of the quadriceps, made by connecting a point near the ASIS to the midpoint of the patella. A typical Q angle is 12 degrees for men and 17 degrees for women. Excessive pronation of the feet can be a contributing factor to this distortion pattern, which is also described as internal knee rotation. This important finding can contribute to injuries in younger patients and degenerative changes as we age.
Bowed Achilles Tendon
In a full weight-bearing position, a foot that pronates excessively will often cause the Achilles tendon to bow medially with the increased eversion of the foot. It’s not uncommon for bowing to be different between the left and right foot, which is consistent with the finding that the amount of excessive pronation is often different between each foot.
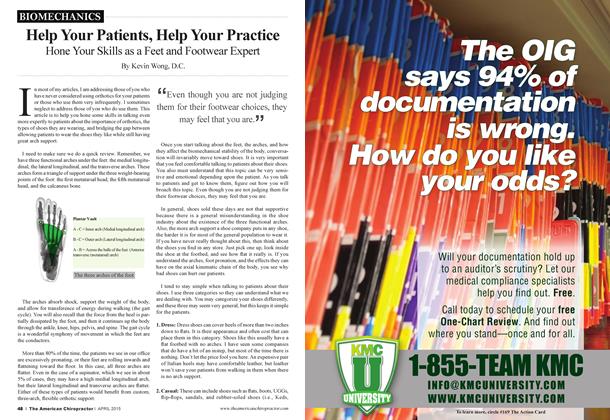
Low Medial Arch
The point of full weight-bearing in the gait cycle is when the foot is fully pronated. Even if the foot “looks” like it has a “good” medial arch, there is a significant chance that there is asymmetry between the feet. This difference in eversion of the calcaneus transmits rotational distortions up into the knee and hip, causing torsion in the pelvis that is nearly ubiquitous. Since low back pain is the number one reason people seek chiropractic care and miss time from work, it seems reasonable to check to see if the feet might be a contributing factor.
Technology now allows us to include 3D laser imaging of the feet in the initial patient evaluation to rule out asymmetrical pronation. That information, along with the visual clues of abnormal shoe wear, excessive foot flare, increased Q angle, and bowed Achilles tendons, gives us quantifiable evidence to justify recommending flexible custom orthotics that support all three arches of the foot as part of a patient’s care plan. Custom orthotics restore optimal foot function and support a healthy gait cycle, thus contributing to the success of chiropractic treatments and optimal patient outcomes.
I was fortunate to have someone watch the way I walked because that person was able to identify some of the silent contributing factors to my chronic low back pain. The success I had with custom stabilizing orthotics modifying my gait and relieving my pain has given me the motivation to include these simple observations in my new patient exams. Our patients deserve to have us “watch the way they walk.”
Dr. Brian Jensen is a graduate of Palmer Chiropractic College and owner of Cave Spring Chiropractic in Roanoke, Virginia. He has been in practice for over 30 years. As a member of the Foot Levelers Speakers Bureau, he travels the country sharing his knowledge and insights. Watch continuing education seminars with Dr. Jensen and other Foot Levelers Speakers at www.footlevelers.com/continuing-education-seminars.