In part one of this series, we looked at arthrogenic muscle inhibition (AMI) of the psoas, describing how this often-overlooked clinical phenomenon can factor into numerous lower body complaints. In part two, we described how psoas AMI is virtually pathognomonic for thoracolumbar (T10-L1) subluxation and covered an effective adjusting technique for this region. Now in part three, we will look at what it takes to fully resolve psoas inhibition and, hence, its effects on the lower body.
A big realization in my learning curve of treating subluxation-induced AMI over the past 20+ years (not just psoas, but in any ‘turned off’ muscle) was that in order to sustainably correct the inhibition you have to sustainably correct its corresponding subluxation(s). It’s fun to adjust someone and see an immediate improvement in muscle strength. However, it’s necessary to discern and address the reason that joint restriction exists in the first place to have a lasting effect and avoid relapse.
An essential aspect to many recurring subluxations, especially those causing inhibition, involves an issue in the soft tissues surrounding the restricted joint. In general, if these soft tissues were completely normal, you’d expect several successful adjustments would fully address the joint restriction and inhibition. However, if the inhibition recurs, there is usually either excessively tight/adhesed myofascia pulling on the area and/or an underlying weakness not keeping these joints stable. We can categorize these as either mobility or stability deficits.
Mobility Considerations
In our psoas inhibition treatment protocol, we’ve created a checklist of the muscles most commonly tight/adhesed that could restrict the thoracolumbar region and cause psoas inhibition. This soft tissue search pattern includes the following:
• Lower thoracic and lumbar paraspinals
• Obliques (lower portion)
• Quadratus lumborum (QL)
• Serratus posterior inferior
• Local semispinalis, multifidi, and rotatores
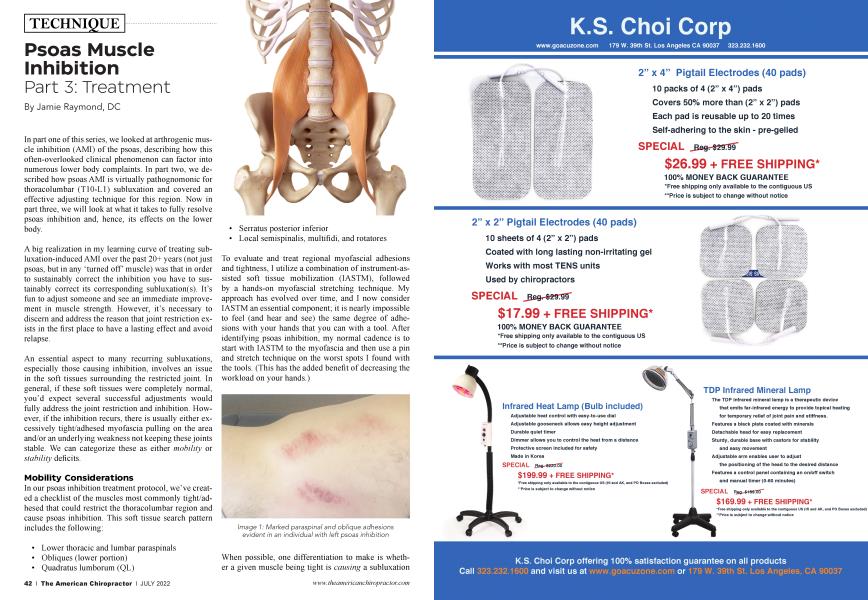
To evaluate and treat regional myofascial adhesions and tightness, I utilize a combination of instrument-assisted soft tissue mobilization (IASTM), followed by a hands-on myofascial stretching technique. My approach has evolved over time, and I now consider IASTM an essential component; it is nearly impossible to feel (and hear and see) the same degree of adhesions with your hands that you can with a tool. After identifying psoas inhibition, my normal cadence is to start with IASTM to the myofascia and then use a pin and stretch technique on the worst spots I found with the tools. (This has the added benefit of decreasing the workload on your hands.)
When possible, one differentiation to make is whether a given muscle being tight is causing a subluxation or is the result of one. For instance, the paraspinals might be adhesed and restricting T12 and its rib, causing a reactive QL spasm. Or the situation also could be completely reversed. IASTM findings are a good indicator — markedly adhesed muscles tend to be more causative. In cases of unilateral psoas inhibition, the tightness/adhesions are typically worse on the side of inhibition. I believe that indicates that the shortened soft tissues are specifically restricting the facet and costovertebral joints more on the affected side.
Despite the order in which I’ve presented these articles, I typically adjust after the soft tissue work because I find it allows for bigger, easier cavitations. (So, scrape, stretch, crack!) My thinking is that, since I know I’m going to do the soft tissue work anyway, I might as well do it first and get as much out of the adjustment as possible. You can find a video covering the ins and outs of this soft tissue work on my YouTube channel.
Stability Considerations
The other category of dysfunction potentially underlying the subluxations that cause recurring muscle inhibition is stability deficits. In the case of the thoracolumbar spine, this means core strength. Core weakness can allow this region to subluxate, inhibiting one or both psoas (and, in a downward spiral, once the psoas is inhibited, core strength is further undermined.)
For the average patient, I consider core strength adequate if they regularly:
• Do a supine abdominal bracing move coupled with hip flexion (e.g., “deadbugs”).
• Include an extension-based exercise such as “bird-dog” or “supermans.”
• Can hold a front plank for 60 seconds and a side plank for 30 seconds.
• Can sit up from a supine position without much difficulty.
• Can bridge off one leg with good form.
• Do some type of resisted hip-abduction exercise.
Athletes who train hard may well need greater core strength. I tell patients this list merely represents a minimum but the more, the better. In fact, you can mitigate the effects of thoracolumbar tightness on the spine and prevent psoas inhibition with enough stability (to a point). It’s good to have baseline routines such as the one above on a handout for your typical runners, hikers, and bikers who love their cardio but not so much core work.
For fit individuals with an otherwise adequate core routine and minimal findings in the mobility screen, psoas inhibition can be a sign of an isolated transverse abdominis (TvA) weakness. This deepest core layer has an important role in maintaining spinal12 (and sacroiliac3) stability. Consequently, even when the other core muscles are strong, an isolated TvA weakness can allow the thoracolumbar spine to subluxate.
TvA is prone to atrophy and reduced activity following such things as an episode of low back pain4 or abdominal surgery5, and doesn’t necessarily recover its strength along with the rest of the core unless the individual is specifically shown an appropriate isolating exercise (also shown on the YouTube video.) An example of this might be a mom with a young child born via c-section, who’s had hip pain since she resumed working out, despite having a good core routine with her trainer.
Differentials
As discussed, when the psoas is testing weak, it’s almost a given that there is thoracolumbar subluxation. So the question then often becomes: does this represent a regional mobility or stability deficit? (Of course, there is no rule that it couldn’t be both.)
In my normal intake, I ask about past traumas and what strength training the person does (looking for any gaps in their core routine). When I find psoas inhibition, all else being equal, I typically start by looking at the region’s mobility and then adjust. If there isn’t much in the way of adhesions and tightness in the regional checklist (or if you’ve already done a few treatments and addressed what was there), it makes it that much more likely that you’re dealing with a stability deficit. If I suspect from the beginning that core or TVA weakness is the primary deficit, I’ll look at the core first. As long as both bases get covered, the order isn’t necessarily critical.
"...does this [thoracolumbar subluxation] represent a regional mobility or stability deficit (or both)?"...
In approaching any lower body injury (including to the lower extremities), I usually get the best results by starting with the thoracolumbar region first. If utilized properly, psoas muscle testing is a quick yet highly predictive component of this evaluation because it is representative of this region’s integrity:
• Psoas inhibition indicates thoracolumbar subluxation and likely a soft tissue mobility and/or stability deficit.
• A lack of psoas inhibition is evidence that the patient has no significant thoracolumbar subluxations and adequate regional mobility and stability. (It also makes it more likely that your patient’s lower body complaint is originating elsewhere — for instance, a weak ankle.)
Expanding the Clinical Picture
As discussed in a previous article, psoas inhibition has a high prevalence in the symptomatic population. While many patients have a weak core, a growing awareness for me over the years has been how often psoas inhibition originates from mobility deficits in the form of thoracolumbar soft tissue adhesions.
Adhesions can result from things such as surgery, structural imbalances, and, especially, trauma. People are forever collidingwith objects, each other, or terra firma. If you look at the mechanics of your average collision, the midto lower-thoracic region bears the brunt of many of these impacts. Additionally, there is absolutely no time limit on adhesions; once they are in place, they can stay there for a person’s lifetime. Consequently, athletes in contact sports, such as football and alpine skiing, can accumulate numerous adhesions in various areas over the years.
It’s been surprising to me to learn how often symptomatic patients have suffered past trauma and how frequently their current injury relates to these older adhesions. (For example, a long-time runner who develops Achilles tendinopathy nine months after falling on the trail and bruising ipsilateral lower ribs.) Quite often, patients won’t link the past trauma to the current injury (or even remember to mention the past trauma during the intake).
Conclusion
In previous articles we described how psoas inhibition, diagnosable by muscle testing and caused most commonly by thoracolumbar subluxation, can contribute to low back, hip, knee, and foot injuries. Linking that thought with this article, we can now say that the root cause of many of these lower body complaints are thoracolumbar mobility and stability deficits, and that these deficits can potentially stem from events years in the past. In these cases, finding and addressing the deficits becomes the key to sustainably solving not only the subluxation and the inhibition it is causing, but also a wide array of lower body complaints.
Jamie Raymond, DC, is a certified chiropractic sports physician and researcher with more than 20 years of clinical experience. He specializes in the causes and effects of muscle inhibition as it relates to musculoskeletal injury and has developed innovative protocols to help other providers incorporate best practice treatments to tackle their most difficult cases. Check out his YouTube channel.
References
1. Barr KP, Griggs M, Cadby T. Lumbar stabilization: core concepts and current literature, Part 1. Am J Phys Med Rehabil. 2005 Jun;84(6):473-80.
2. Hodges PW, Richardson CA. Inefficient muscular stabilization of the lumbar spine associated with low back pain: a motor control evaluation of transversus abdominis. Spine (Phila Pa 1976). 1996 Nov 15;21(22):2640-50.
3. Richardson CA, Snijders CJ, Hides JA, Damen L, Pas MS, Storm J. The relation between the transversus abdominis muscles, sacroiliac joint mechanics, and low back pain. Spine (Phila Pa 1976). 2002 Feb 15;27(4):399-405.
4. Selkow, Noelle M et al. Transversus abdominis activation and timing improves following core stability training: a randomized trial. International journal of sports physical therapy vol. 12,7 (2017): 1048-1056.
5. Shah, Shraddha et al. Altered patterns of abdominal muscle activation during forced exhalation following elective laparotomy: an experimental research. Annals of medicine and surgery (2012) vol. 61 198-204. 9 Dec. 2020, doi: 10.1016/j. amsu. 2020.11.080