FEATURE
PERSPECTIVE
David Seaman
DC
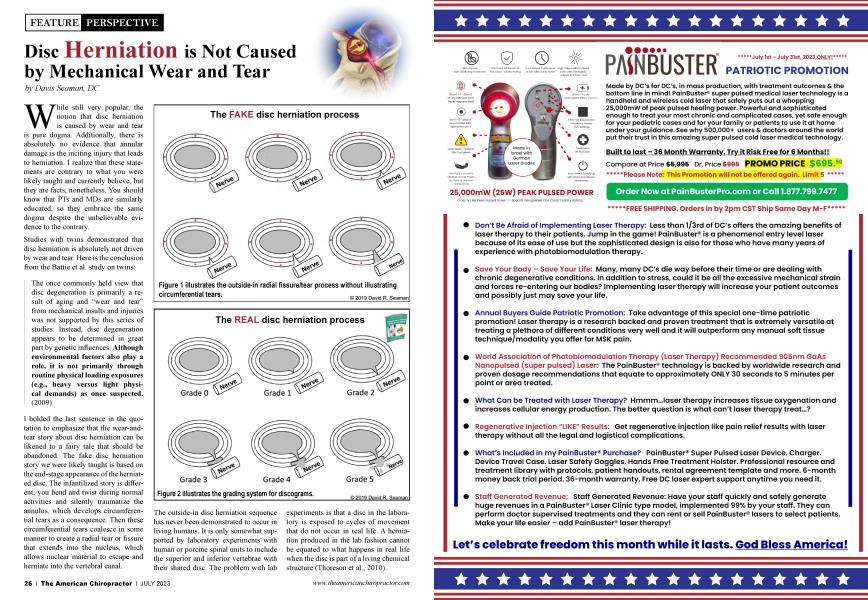
The FAKE disc herniation process
While still very popular, the notion that disc herniation is caused by wear and tear is pure dogma. Additionally, there is absolutely no evidence that annular damage is the inciting injury that leads to herniation. I realize that these statements are contrary to what you were likely taught and currently believe, but they are facts, nonetheless. You should know that PTs and MDs are similarly educated, so they embrace the same dogma despite the unbelievable evidence to the contrary.
Studies with twins demonstrated that disc herniation is absolutely not driven by wear and tear. Here is the conclusion from the Battie et al. study on twins:
The once commonly held view that disc degeneration is primarily a result of aging and “wear and tear” from mechanical insults and injuries was not supported by this series of studies. Instead, disc degeneration appears to be determined in great part by genetic influences. Although environmental factors also play a role, it is not primarily through routine physical loading exposures (e.g., heavy versus light physical demands) as once suspected. (2009)
I bolded the last sentence in the quotation to emphasize that the wear-and tear story about disc herniation can be likened to a fairy tale that should be abandoned. The fake disc herniation story we were likely taught is based on the end-stage appearance of the herniated disc. The infantilized story is different; you bend and twist during normal activities and silently traumatize the annulus, which develops circumferential tears as a consequence. Then these circumferential tears coalesce in some manner to create a radial tear or fissure that extends into the nucleus, which allows nuclear material to escape and herniate into the vertebral canal.
The outside-in disc herniation sequence has never been demonstrated to occur in living humans. It is only somewhat supported by laboratory experiments with human or porcine spinal units to include the superior and inferior vertebrae with their shared disc. The problem with lab experiments is that a disc in the laboratory is exposed to cycles of movement that do not occur in real life. A herniation produced in the lab fashion cannot be equated to what happens in real life when the disc is part of a living chemical structure (Thoreson et al., 2010).
The most important thing to tell patients is that herniated discs should naturally resorb to insignificance over time, which is part of the natural history of disc herniation.
It is important to understand that our body structure is actually a collection of chemicals (protein, fat, carbohydrate, and minerals), so it is technically accurate to refer to the human body as a chemical structure. Our body is chemistry. Despite this fact, we are not taught to view body structure as chemistry; instead, we are taught to view body structure and body chemistry as being different. In short, to ignore chemistry in the context of disc herniation and any other musculoskeletal ailment is to blind oneself from seeing spinal pathology in a legitimate biological context.
For historical orientation purposes, if you do a PubMed search for Adams MA, Hutton WC, you will see papers written as early as 1980 about the disc herniation process. In case you have never heard of Michael Adams, I have heard Stu McGill refer to him as Professor Adams.
Back in the 1980s, Adams took a more annular injury view of disc herniation, but that changed over time to reflect new research finds. For example, on his University of Bristol webpage, Adams states that the title of his 2002 book— The Biomechanics of Back Pain—“does not imply bias towards mechanical explanations of back pain.” This book was coauthored with Nik Bogduk, Kim Burton, and Patricia Dolan. In this book, we are told that the weak link of the lumbar spine is the vertebral endplate, such that when compressive forces are high enough, the first unequivocal sign of disc damage is the endplate—not the annulus (p. 133).
Long before Bogduk coauthored The Biomechanics of Back Pain with Adams, he coauthored a book with Lance Twomey called Clinical Anatomy of the Lumbar Spine, which clearly illustrates how the understanding of disc herniation changed over time. The first edition was published in 1987, in which we are told the following:
Disc herniation is the end result of a combination of factors that may extend over a long period. The initial event is a fracture of an endplate, through which the nucleus pulposus evokes an autoimmune inflammatory response. The fracture may heal, or the inflammatory response may continue relentlessly to degrade more of the nuclear matrix, rendering it expressible. The second requirement is that the annulus develops a radial fissure, most probably as the result of repeated torsional injuries. In the presence of radial fissure, disc material can readily be expelled in the vertebral canal by compressive forces on the nucleus generated during flexion, (p. 144) It was only suggested in the 1987 first edition that torsional injuries were a possible cause of radial Assuring. The second edition was published in 1991, and three pages were devoted to discussing the nuclear degradation process. In contrast with the 1987 edition, which posited that torsional injuries could cause a radial fissure, the 1991 edition provided the updated view:
In time, nuclear degradation extends peripherally to erode the annulus fibrosus, typically along radial fissures. This condition of the disc is known as “internal disruption.” The essence of this condition is that the pathological changes are restricted to the center of the disc. There are no external manifestations of disease in the form of disc bulge, herniation, or loss of disc height. It is an inflammatory condition that involves degradation of the nuclear matrix and progressive erosion of the annulus fibrosus, typically along radial fissures, (p. 169)
Then we are told the following, which is very important, “Ultimately, it is possible for internal disc disruption to progress to disc herniation. This occurs if the inflammatory degradation extends along a radial fissure for the entire thickness of the annulus” (p. 170).
In the 1991 edition, there was no mention of torsional injuries causing radial fissures. Rather, by that time, radial fissures were known to be caused by degradative proteolytic enzymes that progressively erode (digest) annular tissue (p. 168). Back then, the enzymes that degraded collagens were called collagenases, and those that degraded proteoglycans were called stromelysins. Now, they are all called matrix metalloproteinases and are designated by numbers, such as MMP1, which refers to the type of connective tissue that is degraded. In total, there are at least 23 MMPs expressed in human tissue (Laronha & Caldeira, 2020).
If you look up information about MMPs, you will learn that they are the key enzymes involved in extracellular matrix remodeling after exercise and after tissue injury. Their activity is inhibited by tissue inhibitors of metalloproteinases (TIMPs). In other words, discs herniate because MMPs are not inhibited adequately. Before briefly discussing the regulation of MMPs, you need to first visualize the actual herniation process.
While discograms have been discarded as a tool for identifying herniated discs, the grading system allows us to see the herniation sequence. As you can see, disc herniation is an inside-out process, which is initiated by damage to the endplate and the subsequent activation of MMPs, which first degrades the nucleus and then the annulus. I suspect that the reason we have been misled to believe the annular damage outside-in process is because we almost only visualize disc herniation after the herniation has occurred, which causes us to assume that traumatic annular injury is the cause. This does not mean that annular damage does not occur. It does, but that is after the nucleus is degraded and no longer able to bear and distribute compressive loading.
The fact that the disc herniation process occurs in the opposite fashion that you describe to patients does not mean that your treatment approach should change. Depending on the patient, you may get excellent or poor results with manual care, rehabilitation efforts, and electrical modalities. Your results won’t change, but your explanation should be because the false “mechanical injury” story can ultimately function as a source of patient catastrophizing and fear when it comes to engaging in healthy physical activities.
If a patient wants to know how and why discs herniate, tell them that the issue is 70% genetic and 30% environmental (Battie, 2009) (Munir, Rade, Maatta, Freidin, & Williams, 2018). This has been determined by studying twins, such that less than 10% of degenerative changes are explained by occupational loading and physical resistance training (Patel et al., 2011).
After explaining that disc herniation is a combination of genetic and environmental factors, if you choose, the most important thing to tell patients is that herniated discs should naturally resorb to insignificance over time, which is part of the natural history of disc herniation. In the literature, you will see the term “spontaneous resorption.” This is not spontaneous in the common sense of the word; herniated discs can completely resorb at various rates, depending on the patient. The most interesting example of this to me is a 44-year-old medical doctor who suffered through three bouts of herniation and resorption over a 2.3-year period (Reyentovich & Abdu, 2002). The only treatment was anti-inflammatory drugs and staying active. In this case, the L4-L5 disc herniated and resorbed twice.
Fortunately for chiropractors, hyperglycemia and obesity are lifestyle issues, which can be easily and efficiently addressed as a part of a busy chiropractic practice.
This is a great case to use for the purpose of reassuring your patients that they can overcome the pain of disc herniation without surgery.
Between manual and rehabilitative treatments and reassuring the patient, many will readily return to full function. There is also the issue of inflammation to consider. Recall that Bogduk described disc herniation as an inflammatory degradative process. With this in mind, patients with type 2 diabetes are more likely to herniate than age-matched subjects without diabetes. The same holds true for tendinopathy and osteoarthritis because all three conditions are driven by
unregulated MMP activity. It turns out that the hyperglycemic state is associated with less TIMP activity, so less inhibition of MMPs (Seaman, 2020). This is why common musculoskeletal conditions seen by chiropractors are caused by hyperglycemia.
Obesity is an additional driver of disc herniation and not because of excess “mechanical loading.” Rather, the established pro-inflammatory state of obesity is associated with an excess of circulating leptin levels, which can promote disc herniation (Curie, 2020) and also osteoarthritis (OA) (Conde, 2011).
In the case of OA, it has been demonstrated that obese people without excess leptin do not suffer from knee OA, while those with excess leptin do. “This recent finding suggests that obesity, per se, is not a sufficient condition to induce knee OA, but that leptin is necessary in the pathophysiology of OA development and progression associated with obesity.” This is because leptin stimulates MMP activity (Conde, 2011).
With that in mind, it should be obvious that musculoskeletal degeneration is driven by hyperglycemia and obesity, which are both pro-inflammatory states and significant problems suffered by Americans. Approximately 75% of U.S. adults are overweight or obese, and 25% of adults over the age of 18 have metabolic syndrome, the percentage of which increases with age. About 50% of adults 60 years and older have metabolic syndrome, so this is a significant pathological issue that is largely ignored in the context musculoskeletal conditions like disc herniation, OA, tendinopathy, and sarcopenia (Seaman, 2020). Fortunately for chiropractors, hyperglycemia and obesity are lifestyle issues, which can be easily and efficiently addressed as a part of a busy chiropractic practice.
David Seaman, DC, is a consultant for Anabolic Laboratories and has designed several nutritional supplements. He has authored many articles on the topics of diet, inflammation, and pain. His most recent book written for laypeople is The DeFlame Diet. He posts regular DeFlame nutrition updates at DeFlame Nutrition on YouTube and Facebook.
References
1. Battie, M. C., Videman, T., Kaprio, J., Gibbons, L. E., Gill, K., Manninen, EL, Saarela, J., & Peltonen, L. (2009). The twin spine study: Contributions to a changing view of disc degeneration. The Spine Journal : Official Journal of the North American Spine Society, 9(1), 47-59. https://doi.Org/10.1016/j. spinee.2008.11.011
2. Thoreson, O., Ekstrom, L., Hansson, H. A., Todd, C., Witwit, W., Sward Aminoff, A., Jonasson, P., & Baranto, A. (2017). The effect of repetitive flexion and extension fatigue loading on the young porcine lumbar spine: A feasibility study of MRI and histological analyses. Journal of Experimental Orthopaedics, 4(1), 16. https://doi.org/10.1186/s40634... Adams at the University of Bristol.
3. Adams, M.A. Research theme: The biomechanics of back pain. http://www.bristol.ac.uk/anato...
4. Laronha, EL, & Caldeira, J. (2020). Structure and function of human matrix metalloproteinases. Cells, 9(5), 1076. https://doi. org/10.3390/cells9051076
5. Munir, S., Rade, M., Maatta, J. EL, Freidin, M. B., & Williams, F. M. K. (2018). tntervertebral disc biology: Genetic basis of disc degeneration. Current Molecular Biology Reports, 4(4), 143-150. https://doi.org/10.1007/s40610...
6. Patel, A. A., Spiker, W. R., Daubs, M., Brodke, D., & Cannon-Albright, L. A. (2011). Evidence for an inherited predisposition to lumbar disc disease. The Journal of Bone and Joint Surgery. American volume, 93(3), 225-229. https://doi. org/10.2106/JBJS.J.00276
7. Reyentovich, A., & Abdu, W. A. (2002). Multiple independent, sequential, and spontaneously resolving lumbar intervertebral disc herniations: a case report. Spine, 27(5), 549-553. https:// doi.org/10.1097/00007632-200203010-00024
8. Seaman, D. R. (2020). The DeFlame diet to stop your joints, muscles, and bones from rotting. Wilmington: Shadow Panther Press.
9. Curie, G. (2020). tntervertebral disc and adipokine leptin-loves me, loves me not. International Journal of Molecular Sciences, 22(1), 375. https://doi.org/10.3390/ijms22...
10. Conde, J., Scotece, M., Gomez, R., Lopez, V, Gomez-Reino, J. J., & Gualillo, O. (2011). Adipokines and osteoarthritis: Novel molecules involved in the pathogenesis and progression of disease. Arthritis, 2011, 203901. https://doi. org/10.1155/2011/203901